
Air embolism
| Classification according to ICD-10 | |
|---|---|
| T79.0 | Air embolism (traumatic) |
| T80.0 | Air embolism after infusion, transfusion, or injection for therapeutic purposes |
| T81.7 | Postoperative vascular complications, not elsewhere classified Postoperative air embolism, not elsewhere classified |
| O08.2 | Embolism after abortion, ectopic pregnancy and molar pregnancy Air embolism |
| O88.0 | Air embolism during the gestational period |
| ICD-10 online (WHO version 2019) | |
An air embolism is a by the ingress of air into the vascular system caused embolism .
root cause
An air embolism occurs when air enters the bloodstream. It is a special case of gas embolism .
An open connection between a vein and the outside world, provided that there is negative venous pressure (i.e. suction), is sufficient for this to happen. Since such a condition is not usually present in the peripheral veins of the body, complications from simple errors in handling intravenous peripheral indwelling cannulas are rare in the hospital.
The pressure and thus the risk conditions look different with central vein and venous port catheters , because a pulse-synchronous negative pressure is recorded near the heart. Central venous catheter systems open to the environment can therefore be fatal. The use of screw ( Luer lock ) instead of plug connections (Luer without lock) and staff training have made an air embolism rare in this way.
Pressure infusions, such as those used in cardiac catheter examinations , can also lead to a fatal air embolism if the tube system is inadequately ventilated, as several milliliters of air can be pressed directly into the heart or coronary vessels at high pressure. So far there is no technical solution to this problem, so the attention of the staff is the only protection.
The fear of an air embolism is historically associated with thyroid surgery (possible opening of the neck of the neck) at a time when no intubation anesthesia was known, which is associated with completely changed pulmonary pressure values and thus increased venous pressures. In this case, you protected yourself by lying slightly head-down on the operating table (Kocher).
Air embolism is related to caisson disease in terms of its cause (gas) and to pulmonary thrombembolism in terms of its consequences for the heart .
Symptoms
The signs of an air embolism are similar to those of a pulmonary embolism , that is
- Painful breathing
- to cough
- Decrease in the oxygen content of the blood with shortness of breath and accelerated breathing
- Shock (drop in blood pressure, accelerated pulse ) with possibly loss of consciousness
- Fear , possibly also panic due to shortness of breath, possibly with profuse sweating
Diagnosis
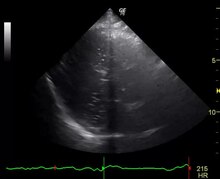
In addition to the clinical picture, the air can be detected directly in the heart ultrasound . The EKG can show changes as in a heart attack . The blood gas analysis may show a drop in the oxygen content.
therapy
As the most important measure, the cause of the air embolism must be eliminated immediately, i.e. the further inflow of air into the circulation must be prevented. Depending on the severity of the symptoms, it may be necessary to ventilate the patient. Air can sometimes be sucked out of the right atrium through a central venous catheter .
In order to avoid further embolization of the lungs, the patient should be placed in the left side position with the head down ( Durant maneuver ). As a result, the air should remain in the right ventricle and no longer reach the pulmonary circulation.
A resuscitation may be necessary, possibly circulatory stabilizing measures have to be taken.
Individual evidence
- ↑ W. Böcker, H. Moch: Pathology. Elsevier and Urban & Fischer Verlag, 2008, ISBN 3-437-42382-7 , p. 237 ( limited preview in the Google book search).
- ↑ Joachim Gabka: Injection and Infusion Technology: Practice, Complications and Forensic Consequences. 4th edition, De Gruyter, Berlin 1988, ISBN 3-11-011000-8
- ↑ E. Türk, N. Schulz, K. Püschel: Air embolism when performing a coronary angiography. In: Rechtsmedizin 17, 2007, pp. 215–217.
- ↑ Federal Institute for Drugs and Medical Devices (BfArM): Air embolism through contrast agent injectors. News from September 18, 2007; Reference no. 2198/04