
Primary insomnia
| Classification according to ICD-10 | |
|---|---|
| F51.0 | Inorganic Insomnia |
| ICD-10 online (WHO version 2019) | |
The primary insomnia (Syn. Agrypnie , insomnia ) is one of the sleep disorders and is characterized, in contrast to the secondary shape, by the absence of an organic or psychiatric disorder is selected from.
Epidemiology
If the diagnostic criteria of DSM-IV and ICD-10 are strictly followed , primary insomnia has a prevalence of around 3% in the general population. Women are more often affected than men. If one considers non-organic sleep disorders with or without daytime sleepiness, regardless of the criteria, the prevalence is up to a third of the total population.
Etiopathogenesis
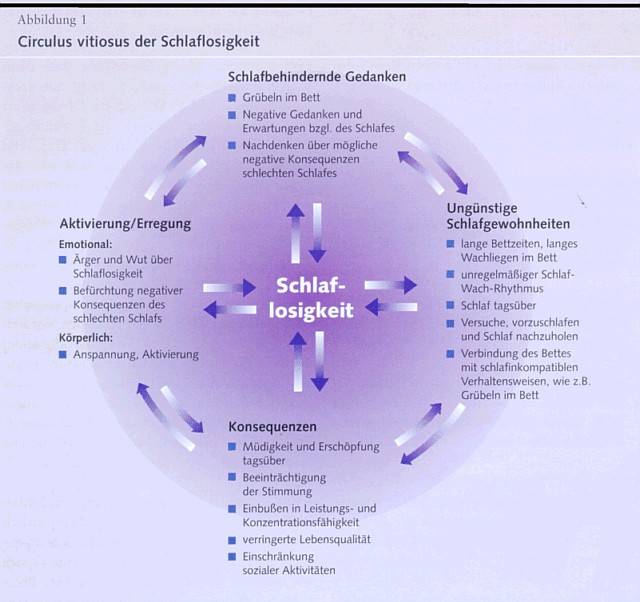
Primary insomnia is usually based on a triggering life event. This either leads to sleep-impairing thoughts or to activation or arousal and then sets a corresponding vicious circle in motion. Unfavorable sleeping habits can also set this vicious circle in motion.
It can start with thoughts that are disturbing sleep (brooding, negative thoughts, thinking about the negative consequences of poor sleep). This then continues with increased tension or excitement (emotional, motor, autonomous nervous system). The consequence of this is fatigue, a bad mood, a decline in concentration and productivity, reduced activity in life or restricted social contacts. This promotes unfavorable sleeping habits such as long bed times, long lying awake, irregular sleep-wake rhythm or daytime sleep. This then results in thoughts that are disturbing sleep and consequently maintain this cycle of primary insomnia. This also makes it very clear why primary insomnia is chronic and has long-term consequences.
clinic
According to the DSM-IV diagnostic criteria, primary insomnia presents itself as follows:
- Predominant complaints related to difficulty falling asleep or staying asleep for at least one month,
- the insomnia and the associated daytime sleepiness lead to significant impairments in important areas of life,
- the sleep disorder is not solely due to another sleep disorder,
- the sleep disorder did not occur in the course of a psychiatric illness (e.g. major depression, anxiety disorders, etc.),
- the sleep disorder is not the result of medication, drug use or an underlying organic disease.
The risk of developing depression is increased in patients with primary insomnia.
Diagnosis
Several standardized measuring instruments in the form of questionnaires are available for assessing sleep quality or daytime sleepiness, such as the Pittsburgh Sleep Quality Index (PSQI). Keeping a sleep diary by the patient for one to two weeks is groundbreaking for diagnosis and therapy decisions . Among other things, bed times as well as sleeping and waking phases are logged. With the help of an actigraphy , the sleeping times can be roughly objectified. Polysomnography can also be performed in a sleep laboratory to rule out other sleep disorders or if there is no response to therapy . In any case, a physical and psychological / psychiatric history should be taken.
therapy
Non-drug procedures
Measures to improve sleep hygiene (e.g. maintaining a constant sleep-wake cycle, avoiding alcohol and caffeine), stimulus control (Bootzin, 1971) and sleep restriction (Spilman, Saskin and Thorpy, 1987) have proven effective. The sleep restriction is about shortening the awake time in bed, which is why one should not speak of sleep restriction, but rather of the "restriction of time in bed". Depending on the patient's specific problems, various relaxation methods can also be used (e.g. progressive muscle relaxation according to Jacobson, autogenic training ). In addition to these behavior control measures, cognitive techniques are also used, the aim of which is to reduce sleep-impairing thoughts.
Medicinal procedures
There are sleeping pills used. Benzodiazepines can be administered for short-term therapy. In the longer term, however, problems arise with this medication due to the long half-life, the withdrawal effects and the development of tolerance and dependence. The so-called “Z-preparations” ( zopiclone , zolpidem , zaleplon ) are available as alternatives , which have a shorter half-life and should have a more favorable side effect profile. However, there is still no reliable evidence of this. Sedating antidepressants (e.g. mirtazapine , trimipramine , trazodone ) are a good option, especially for long-term therapy, but are off-label for use as sleeping pills. First generation anti-histamines can be prescribed as hypnotics thanks to their CNS penetrability.
literature
- M. Berger (Ed.): Mental illnesses. Clinic and Therapy. 3. Edition. Urban & Fischer, 2009, ISBN 978-3-437-22481-2 .
- PJ Hauri: Behavioral Therapy for Sleep Disorders. In: K. Meier-Ewert, H. Schulz (Ed.): Sleep and sleep disorders. Springer, Berlin 1989, ISBN 3-540-52073-2 .
- M. Kryger et al. a. (Ed.): Principles and Practice of Sleep Medicine. 4th edition. Saunders, 2005, ISBN 1-4160-0320-7 .
- H.-J. Möller, D. Laux, A. Deister: Psychiatry and psychotherapy. 4th edition. Thieme, 2009, ISBN 978-3-13-128544-7 .
Web links
- S1 guideline insomnia of the German Society for Neurology. In: AWMF online (as of 2008) (PDF)
Individual evidence
- ^ Roche Lexicon Medicine . 5th edition. Elsevier, Urban & Fischer Verlag, Munich 2003, ISBN 3-437-15072-3 (keyword: insomnia, insomnia).
- ↑ Hildegard Kaulen: Lack of sleep - illness without definition. In: Frankfurter Allgemeine Zeitung. February 16, 2012, accessed August 2, 2012 .
- ^ MM Ohayon: Epidemiology of insomnia: what we know and what we still need to learn. In: Sleep Medicine Reviews . 2002; 6, pp. 97-111.
- ↑ vicious circle of insomnia. (JPEG) Retrieved June 14, 2010 .
- ↑ H.-J. Möller, D. Laux, A. Deister: Psychiatry and psychotherapy . 4th edition. Thieme Verlag, Stuttgart 2009, ISBN 978-3-13-128544-7 , p. 293-306 .
- ^ Diagnostic and Statistical Manual of Mental Disorders. 4th edition. American Psychiatric Association, APA, Washington 1994.
- ^ D. Riemann, U. Voderholzer: Primary insomnia: a risk factor to develop depression? In: Journal of Affective Disorders. (2003); 76, pp. 255-259.
- ↑ Diagnosis and therapy of sleep disorders. (PDF; 242 kB) (No longer available online.) Hirslanden Private Hospital Group, archived from the original on March 7, 2016 ; Retrieved October 9, 2012 . Info: The archive link was inserted automatically and has not yet been checked. Please check the original and archive link according to the instructions and then remove this notice.
- ^ Nils Heim: The role of polysomnography in the diagnosis of insomnia. (PDF; 1243 kB) University of Freiburg, October 15, 2010, accessed on October 9, 2012 .
- ↑ a b DGN guidelines - Insomnia. (PDF; 143 kB) German Society for Neurology, accessed on October 9, 2012 .
- ↑ Jürgen Staedt, Dieter Riemann: Diagnostics and therapy of sleep disorders . W. Kohlhammer Verlag, 2006, ISBN 978-3-17-019467-0 , pp. 187 ( google.de [accessed on July 9, 2017]).
- ^ Matthias Berking, Winfried Rief: Clinical Psychology and Psychotherapy for Bachelor: Volume I: Basics and Disorder Knowledge. Read, listen, learn on the web . Springer-Verlag, 2012, ISBN 978-3-642-16974-8 , pp. 209 ( google.de [accessed on July 9, 2017]).
- ↑ Hauri: Behavioral Therapy for Sleep Disorders. 1989, pp. 147-155.
- ↑ Jürgen Staedt, Dieter Riemann: Diagnostics and therapy of sleep disorders . W. Kohlhammer Verlag, 2006, ISBN 978-3-17-019467-0 , pp. 155 ( google.de [accessed on July 9, 2017]).
- ↑ Jürgen Margraf, Silvia Schneider: Textbook of behavior therapy: Volume 2: Disorders in adulthood - Special indications - Glossary . Springer Science & Business Media, 2008, ISBN 978-3-540-79542-1 , p. 208 ( google.de ).
- ↑ Non-drug therapy for insomnia. Sleep Medicine Center Munich, accessed on October 9, 2012 .
- ↑ D. Riemann, ML Perlis: The treatments of chronic insomnia: a review of benzodiazepine receptor agonists and psychological & behavioral therapies. In: Sleep Medicine Reviews. (2009).
- ↑ Pharmacological treatment of insomnia. Sleep Medicine Center Munich, accessed on October 9, 2012 .
- ↑ Show intuition and sensitivity. In: Pharmaceutical newspaper. 2009, accessed October 9, 2012 .
- ↑ Insomnia. (PDF; 5641 kB) In: Österreichische Ärztezeitung. October 25, 2010, pp. 44–45 , accessed October 9, 2012 .
{kind=link}