
Primary biliary cirrhosis

| Classification according to ICD-10 | |
|---|---|
| K74.3 | Primary biliary cholangitis Chronic non-purulent destructive cholangitis |
| ICD-10 online (WHO version 2019) | |
The primary biliary cholangitis ( PBC , chronic non-suppurative destructive cholangitis, formerly primary biliary cirrhosis) is a relatively rare autoimmune disease of the liver that affects about 90% of cases women. This begins (primarily) in the small bile ducts (biliary), which are destroyed by inflammation. In the longer term, the inflammation can spread to the entire liver tissue and lead to scarring. Since cirrhosis can only occur in the end-stage of the disease , the name was changed in the specialist literature from 2015 to "Primary biliary cholangitis". The disease can be z. B. by the detection of antimitochondrial antibodies (AMA) in the blood can already be detected when the liver is still relatively intact.
Symptoms
Particularly common symptoms of PBC are tiredness and exhaustion (70–90% of patients) and itching (20–70%). Rheumatism- like side effects include joint problems, thyroid diseases (Hashimoto's thyroiditis) and dry mucous membranes ( Sicca syndrome ). Small fat deposits in the inner corners of the eyes ( xanthelasma ) are observed in approx. 20% of patients. Fat stools and vitamin deficiencies (especially vitamins A, D, E and K) can also be associated with PBC. Recurring urinary tract infections were found in 20% of women with PBC . In the late stage of cirrhosis, typical cirrhosis complications can arise (see cirrhosis ). These include water belly ( ascites ), varicose veins in the esophagus ( esophageal varices ) or in the stomach ( fundic varices ), disorders of brain function ( hepatic encephalopathy ) and liver cancer. However , new research results question whether PBC also increases the risk of bone loss ( osteoporosis ).
diagnosis
General laboratory values that can indicate inflammation of the biliary tract or biliary blockage are often elevated: These include alkaline phosphatase (AP) and gamma-glutamyl transpeptidase (GGT or Gamma-GT). If the liver is damaged, the liver enzymes AST and ALT are also increased; in the course of the process, the coagulants synthesized by the liver can fall, so that the bleeding time increases, i.e. the Quick value decreases. The protein compound IgM (antibodies) can be increased in PBC.
The so-called antimitochondrial antibodies (AMA) of the M2 subtype are increased in the blood in 90% of PBC patients . This finding can often prove the diagnosis. (A rare exception without an increase in AMA is the so-called "AMA-negative PBC", which is also known as autoimmune colangitis.) Other PBC-specific antinuclear antibodies (ANA) are directed against nuclear dots (sp100) and nuclear membrane (gp210.) ).
In the early stages of ultrasound (sonography), the liver can look normal or similar to fatty liver . In later stages the liver can be enlarged, in the final stage of cirrhosis the surface is often bumpy or wavy, and the liver can shrink again here.
A liver puncture ( liver biopsy ) can help with the initial diagnosis and confirm the diagnosis with a tissue examination.
It is important to clear the PBC from other autoimmune diseases such as B. autoimmune hepatitis or primary sclerosing cholangitis . In up to 10% of cases, mixed forms such as B. PBC and autoimmune hepatitis occur (so-called overlap syndrome).
causes
The causes and triggers of PBC are now known. Studies suggest that it is an autoimmune disease . This means that the own immune system can no longer differentiate between "foreign" and "own" due to a defect and attacks the mitochondria in the body's own cells. The corresponding autoantibodies are directed against the E2 subunit of the pyruvate dehydrogenase complex , the enzyme dihydrolipoyl transacetylase .
Opinions differ greatly as to which other factors can cause PBC to break out. Discussions include a. hormonal and genetic influences, medication, infections with viruses, fungi or bacteria as well as environmental influences. One study indicated that E2 derivatives, in which lipoic acid was replaced by octyne-7-carboxylic acid , a compound used as a methyl ester industrially as a fragrance and flavor ( violets ), the modified E2 had a much stronger antigenic effect. Allergies to the methyl ester are known. Cosmetic articles with this substance must be labeled EU-wide ("METHYL 2-OCTYNOATE").
The influence of pregnancy on PBC and vice versa of PBC on pregnancy has not been clarified. Alcohol has not been shown to cause PBC. However, as with all liver diseases, it can adversely affect the course and should be strictly avoided.
Today's therapy
If left untreated, PBC can lead to death within about twelve years, but the course varies from patient to patient and life expectancy does not appear to be significantly reduced in the early stages of the disease. The standard therapy for PBC today consists of ursodeoxycholic acid (UDCA), which can be given as a tablet. Therapy is usually well tolerated, starts after diagnosis, and lasts for life. The aim of the therapy is to slow down the course of the disease and to improve laboratory values.
transplantation
If the disease progresses to decompensated cirrhosis despite therapy or symptoms such as If itching is unbearable for patients despite treatment, a liver transplant is often necessary. In 75% of the transplanted patients the PBC is cured, in 25% PBC-like damage can develop again in the new liver. After a successful liver transplant, the long-term prognosis for PBC patients is good.
Future prospects
A breakthrough in the search for the cause of the PBC is hardly to be expected in the coming years either. Many studies seem plausible in themselves, but contradict each other in the results. Reports in the medical press that the cause has been found (e.g. environmental influences or retroviruses) should therefore be taken with great caution.
In order to further improve the therapy of PBC, studies are currently being investigated whether the combination of ursodeoxycholic acid (UDCA) with corticosteroids works better than UDCA alone. The final results are still pending; the combination therapy is currently not approved in Germany (as of May 2008).
Picture gallery
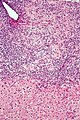
Microphoto of primary biliary cirrhosis ( HE staining , medium magnification).

Photomicrograph of primary biliary cirrhosis (HE stain, low magnification).


See also
Individual evidence
- ↑ A. Lleo, C. Selmi, P. Invernizzi et al. a .: Apotopes and the biliary specificity of primary biliary cirrhosis . In: Hepatology . tape 49 , no. 3 , March 2009, p. 871-879 , doi : 10.1002 / hep.22736 , PMID 19185000 .
- ↑ K. Amano, PS Leung, R. Rieger a. a .: Chemical xenobiotics and mitochondrial autoantigens in primary biliary cirrhosis: identification of antibodies against a common environmental, cosmetic, and food additive, 2-octynoic acid . In: J. Immunol. tape 174 , no. 9 , May 2005, p. 5874-5883 , PMID 15845458 ( jimmunol.org ).
- ↑ JS English, RJ Rycroft: Allergic contact dermatitis from methyl heptine and methyl octine carbonates . In: Contact Dermatitis . tape 18 , no. 3 , March 1988, p. 174-175 , PMID 2966714 .
- ↑ Labeling of fragrances. In: bund.de. BVL , accessed on February 13, 2017 .
swell
- U. Leuschner: Autoimmune diseases of the liver and overlap syndromes. 1st edition. UNI-MED Verlag, 2001.
- H. Rautiainen et al. a .: Budesonide Combined with UDCA to Improve Liver Histology in Primary Biliary Cirrhosis: A Three-Year Randomized Trial. In: Hepatology , April 2005, pp. 747-752.
- AS Abdulkarim, LM Petrovic, WR Kim, P. Angulo, RV Lloyd, KD Lindor: Primary biliary cirrhosis: an infectious disease caused by Chlamydia pneumoniae? In: J Hepatol . , 2004 Mar, 40 (3), pp. 380-384.
- K. Dohmen et al. a .: Atrophic corpus gastritis and Helicobacter pylori infection in primary biliary cirrhosis. In: Dig Dis Sci. , 2002 Jan, 47 (1), pp. 162-169.
- M. Durazzo et al. a .: Lack of association between seroprevalence of Helicobacter pylori infection and primary biliary cirrhosis. In: World J Gastroenterol. , 2004 Nov 1, 10 (21), pp. 3179-3181.
- A. Floreani, A. Mega, V. Camozzi, V. Baldo, M. Plebani, P. Burra, G. Luisetto: Is osteoporosis a peculiar association with primary biliary cirrhosis? In: World J Gastroenterol. , 2005 Sep 14, 11 (34), pp. 5347-5350.
- M. Gershwin et al. a .: Apocalypsal versus Apocryphal: The Role of Retroviruses in Primary Biliary Cirrhosis. In: American Journal of Gastroenterology . Volume 99, Issue 12, December 2004, p. 2356.
- R. Klein, M. Wiebel, S. Engelhart, PA Berg: Sera from patients with tuberculosis recognize the M2a-epitope (E2-subunit of pyruvate dehydrogenase) specific for primary biliary cirrhosis. In: Clin Exp Immunol. , 1993 May, 92 (2), pp. 308-316. Related Articles, Links
- PS Leung u. a .: Is there a relation between Chlamydia infection and primary biliary cirrhosis? In: Clin Dev Immunol. , 2003 Jun-Dec, 10 (2-4), pp. 227-233.
- HY Liu et al. a .: The relationship between Chlamydia pneumoniae infection and primary biliary cirrhosis. In: Zhonghua Gan Zang Bing Za Zhi , 2004 Sep, 12 (9), pp. 546-548.
- AL Mason et al. a .: Pilot studies of single and combination antiretroviral therapy in patients with primary biliary cirrhosis. In: Am J Gastroenterol. , 2004 Dec, 99 (12), pp. 2348-2355.
- HT Sørensen u. a .: Risk of primary biliary liver cirrhosis in patients with celiac disease: Danish and Swedish cohort data. In: Gut , (May) 1999, 44, pp. 736-738.
- L. Vilagut et al. a .: Antibodies to mycobacterial 65-kD heat shock protein cross-react with the main mitochondrial antigens in patients with primary biliary cirrhosis. In: Eur J Clin Invest. , 1997 Aug, 27 (8), pp. 667-672. Related Articles, Links
- L. Xu et al. a .: Cloning the human betaretrovirus proviral genome from patients with primary biliary cirrhosis. In: Hepatology , 2004 Jan, 39 (1), pp. 151-156.
- T. Kumagi, EJ Heathcote: Primary biliary cirrhosis . In: Orphanet J Rare Dis. , 2008 Jan 23, 3, p. 1. PMID 18215315