
Cruciate ligament

The cruciate ligaments ( Latin : Ligamenta cruciata genus ) belong to the ligamentous apparatus of the knee joint in mammals , along with the outer ligament ( Ligamentum collaterale fibulare ) and the inner ligament ( Ligamentum collaterale tibiale ) . They cross in the center of the knee joint, which is why they get their name. Its task, together with the other structures of the knee ligament apparatus, is to stabilize the joint with every movement.
anatomy
Strictly speaking, and purely anatomically, the cruciate ligaments are not located in the knee joint, but outside the joint surfaces ( extra-articular ). This is due to the fact that they are separated from the joint surfaces by the joint mucous membrane sac ( synovial sac ). This synovial sac only encloses the anterior and lateral parts of the cruciate ligaments with its outside, which is why it is referred to as a retrosynovial position . Historically it has been established that the cruciate ligaments radiate into the joint area from behind and not the other way around, which explains their location outside the synovial membrane.
structure
The cruciate ligaments, like other ligaments that accompany the joint, consist of tight, collagenous fibers. They lie parallel to each other in so-called fiber bundles, which are loosely connected to each other by connective tissue. Where they attach to the bone ( insertion ), their fiber structure and arrangement changes in the direction of the periosteum , which also consists of very tight collagen fibers, which are, however, strongly networked. They receive their blood supply primarily from the A. genus media .
Location and course
Anterior cruciate ligament
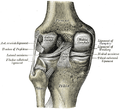
If you open a knee joint from the front, you can see that the cruciate ligaments are located centrally in the joint . The anterior cruciate ligament ( ligamentum cruciatum anterius , ACL or LCA or ACL) is fixed in the anterior-middle area of the knee joint ( area intercondylaris anterior ) to the two cartilage-free cruciate ligament cusps ( tuberculum intercondylare mediale / lateral tibiae ) of the tibial head ( caput tibiae ). This raised area between the two articular surfaces of the tibial head is called the intercondylar eminentia . This is where not only the anterior cruciate ligament starts, but also the fibers of the two menisci. The ligament runs from the front-bottom-inside (anterio-caudal-medial) into the pit between the articular knots ( fossa intercondylaris femoris ) to the rear-top-outside (dorso-cranial-lateral). There it inserts ( insertion = bony ingrowth of tendons and ligaments ) in the rear area of the surface of the outer femoral joint knot facing the middle ( condylus lateralis femoris ) at the cartilage-bone border . This course is also known colloquially as "pocket-shaped".
There are three parts of the tape:
- An anterior-inner ( anteromedial ) bundle. This has the longest fibers of the entire anterior cruciate ligament. When looking into the knee joint from the front, it is the first to be seen. It is particularly tight when the knee is bent ( flexion ). If the anterior cruciate ligament is injured, it is the portion that is most likely to tear.
- A posterior-outer ( posterolateral ) bundle. This is covered by the anteromedial bundle and has its maximum tension when the knee is extended ( extension ). If the ligament is partially torn , it usually remains intact.
- An intermediate bundle.
The fibers have different lengths between 18.5 and 33.5 mm. The bundles fan out for each insertion on the femur and tibia, which increases the area of the fixation. Overall, the ribbon is stretched in itself and the individual bundles are twisted in a slightly spiral shape, which is why the ribbon can be seen as an almost round, thick structure towards the middle. Some fiber strands do not insert into the bone, but rather pull to the anterior medial meniscus ligament , with which they then grow into the bone.
Posterior cruciate ligament
The posterior cruciate ligament appears behind the anterior cruciate ligament ( ligamentum cruciatum posterius , HKB or LCP, in clinical practice often also PCL, English posterior cruciate ligament). It crosses the anterior cruciate ligament at an angle of approx. 90 ° with the knee bent. It is stronger and represents the strongest ligamentous structure of the knee joint. It is in the rear ( dorsal ) area of the area between the articular cartilage of the tibial bone ( area intercondylaris posterior ) on the tibial head, but not like the anterior cruciate ligament on the tibial one Plateau, but fixed at the rear edge (beginning about 10 mm below the joint surfaces). The fixed point of the tibia is thus far behind the posterior horns of the inner and outer meniscus. The ligament runs from the back-bottom-outside (dorso-caudal-lateral) to the front-top-inside (antero-cranial-medial) into the entire depth of the pit between the articular knots (condyles) of the thigh bone. It inserts there at the inner area of the cartilage-bone border of the inner joint knot ( condylus medialis femoris ). With a knee flexed 90 °, looking from the inside, one could see the fan-shaped insertion from 12 o'clock to 4 or 5 o'clock.
Two parts of the tape can be distinguished:
- A posterior-inner (posteromedial) bundle (PM bundle), which has the innermost point of attachment on the back of the shin and the deepest and thus rearmost (with the knee extended) on the femur. The PM bundle reaches its maximum tension when the knee joint is fully extended.
- An anterior-outer (anterolateral) bundle (AL bundle), which extends from the shin to the highest and thus foremost attachment point on the femur. The AL bundle is fully tensed when the knee joint is flexed approximately 90 °.
It is not uncommon for the posterior cruciate ligament to be accompanied by one or two irregularly occurring ligaments, which for a long time have been considered an integral part of the posterior cruciate ligament: the more common posterior meniscofemoral ligament ( ligamentum meniscofemorale posterior, Wrisberg ligament ), which together with the ligament of the posterior horn of the outer meniscus is inserted on the tibia, and the somewhat rarer anterior meniscofemoral ligament ( ligamentum meniscofemorale anterior, Humphry ligament ). In fact, both are not physiologically fused with the fiber strands of the cruciate ligament and do not change anything in the overall structure of the actual posterior cruciate ligament, which is why they must not be seen as a cruciate ligament component, but as an anatomically irregular additional stabilization.
Posterior cruciate ligament in the dorsal view (from behind)
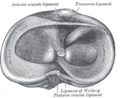
Tibial insertions of the cruciate ligaments and the Wrisberg ligament


Orientation of the cruciate ligaments

When viewed from a perspective, the cruciate ligaments actually cross. They are also crossed in the sagittal plane , the anterior cruciate ligament runs obliquely upwards and backwards, while the posterior cruciate ligament is oriented obliquely upwards and forwards (the anterior cruciate ligament runs laterally past the posterior cruciate ligament). Their course is also crossed in the frontal plane : their attachments on the shinbone lie on a sagittal axis, while the fixed points on the femur are approx. 17 mm apart. The posterior cruciate ligament consequently runs diagonally upwards-centered (cranial-medial), the anterior cruciate ligament diagonally upwards-laterally (cranial-lateral). In the transversal plane, however, they are parallel to one another, their axial sides touching one another. The cruciate ligaments not only cross each other, but also the opposite ipsilateral collateral ligament (collateral ligament). The anterior cruciate ligament crosses the collateral ligament of the fibula and the posterior cruciate ligament that of the tibia. If you look at the four bands from the middle to the side or vice versa, you can see that they are alternately oriented obliquely to one another. The lateral and cruciate ligaments intersect at one point (viewed as projected) in every position of the joint; the intersection corresponds to the current center of rotation.
The two cruciate ligaments have a different incline. With the knee extended, the anterior cruciate ligament is more vertical and the posterior cruciate ligament more horizontally, which corresponds to the alignment of the insertion fields. The field of the posterior cruciate ligament is horizontal, that of the anterior cruciate ligament is vertical.
If the knee is bent, the posterior cruciate ligament, lying horizontally in the extended position, stands up vertically. It describes an arc of more than 60 ° in relation to the tibia, while the position of the anterior cruciate ligament changes only slightly.
The length ratio between the cruciate ligaments varies from person to person. The distance between the fixed points of the shin and thigh bone is characteristic of every knee, a. determine the profile of the rolling hills.
function
The cruciate ligaments together with the collateral ligaments hold the knee joint together. They limit the extension of the shin, guide the joint during movement and thus give it the necessary stability. The lateral stability of the two side ligaments prevents a bow-leg ( genu varum ) or a knock-leg ( genu valgum ). Thus, they represent the central component in the proprioceptive control loop of the knee joint.
The cruciate ligaments form the central passive guide elements of the knee joint. Due to their position in relation to one another and their type of fixation on the thighbone and shinbone, they form a four-bar chain and thus force the head of the thighbone into a roll-slide mechanism ( athrokinematics or osteokinematics ) during flexion , which - among other mechanisms - allows one large articular head to move physiologically on a much smaller socket. If the anterior cruciate ligament is damaged, it is severely disturbed and leads to cartilage and meniscus damage . The cruciate ligaments provide, in addition to the contact pressure of the two joint partners, among other things, a movable stabilization forwards and backwards. They lie in such a way that parts of them are stretched in almost all positions of the knee joint; In the endangered unstable flexion position, in which the collateral ligaments slacken, they prevent an anterior and posterior displacement of the connected (articulating) surfaces. The collateral ligaments are tightened in extension by the spiral shape of the rolling hills of the thigh bone, because the distance between the origin and insertion becomes longer. They are loose in flexion, analogous to the stable or unstable joint surface shape in extension and flexion. If the rolls of the femur were round, the radius would be the same in every flexion angle and the ligaments would pull with constant tension. The extended knee is stable, when bent it is mobile and relieved. The anterior cruciate ligament limits the stretching ( extension ) of the knee joint. In the stretching direction, the rear-lateral and intermediate bundles are most tense, while in the bending direction ( flexion ) the front-central bundle is more tense. The posterior cruciate ligament prevents a straight posterior displacement ( translation ) of the tibial head. In addition, they limit the rotational movement (by the stability and the course direction of their strong fibers rotational movement a) of the lower leg, in particular the rotational movement to the inside.
If the thigh bone rotates outwards and the lower leg inwards (i.e. a twisting movement of the shin inwards), the cruciate ligaments are tightened. They loop around each other to a greater extent and thus attract each other, while they roll out again and loosen as they rotate outwards.
The axis of rotation must run through the inner meniscus because it has grown together with the inner collateral ligament and therefore cannot slide. Tight ligaments are the prerequisite for good joint stabilization. Through the alternating alternation of flexion and extension, of screwing and unscrewing, the ligaments are alternately put under tension and relieved again. Tension and relief optimize the structural organization within the ligaments and promote the metabolism .
Cruciate ligament tear

Cruciate ligament injuries are mostly caused by indirect violence. A tear ( rupture ) of the cruciate ligament is a partial or complete tear of one or both cruciate ligaments. In extreme cases, it is a complete tear or tear, which can also affect parts of the bone. The bony tear or avulsion is much rarer than the pure ligament tear without bony involvement (intraligamentary rupture).
literature
- Antje Hüter-Becker: Textbook on the new thinking model of physiotherapy - Volume 1 movement system , Thieme Verlag, Stuttgart, New York 2002
- Kurt Tittel: Descriptive and functional human anatomy , 12th, completely revised edition, Fischer Verlag, Jena, Stuttgart 1994
- Michael J. Strobel, Andreas Weiler: Hinteres Kreuzband , 1st edition, Endo Press (kindly recommended by Karl Storz Endoskope), 2008, ISBN 978-3-89756-719-1
- Andreas Ficklscherer: BASICS Orthopedics and Trauma Surgery. Elsevier, 2012, ISBN 978-3-437-42208-9 .
Individual evidence
- ↑ Herbert Lippert: Textbook Anatomy , 6th edition, Urban and Fischer, Munich / Jena 2003, ISBN 3-437-42361-4 .
- ↑ B. Tillmann: On the functional morphology of joint development , In: Orthopädische Praxis , No. 12, 1974, pp. 328–342.
- ↑ a b c d Michael J. Strobel, Andreas Weiler: Hinteres Kreuzband , 1st edition, Endo Press (with the kind recommendation of Karl Storz - Endoskope), 2008, ISBN 978-3-89756-719-1 .
- ↑ a b c Hans-Joachim Appell, Christiane Stang-Voß : Functional Anatomy , 4th edition, Springer Verlag, 2008, ISBN 978-3-540-74862-5
- ↑ HE Cabaud: The biomechanics of the anterior cruciate ligament , In: Journal of Orthopedics. , 1984 ed. 2, pp. 105ff.
- ↑ CM Gupte et al .: A review of the functions and biomechanics of the meniscofemoral ligaments , In: Arthroscopie , Edition 19, 2003, pp. 161-171