
Endemic syphilis
| Classification according to ICD-10 | |
|---|---|
| A65 | Endemic Syphilis - Non-Venereous Syphilis - Bejel - Njovera |
| ICD-10 online (WHO version 2019) | |
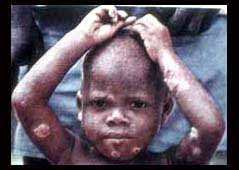
The endemic syphilis or Bejel is a bacterial infectious disease of man, caused by the bacterium Treponema pallidum ssp. endemica is caused. In contrast to true syphilis caused by Treponema pallidum ssp. pallidum , Bejel is not transmitted sexually ( venereally ), but rather through smear infection in close social contact, preferably under socio-economically poor conditions. Therefore, Bejel is also known as non-veneric syphilis . It occurs preferentially in children between 4 and 10 years of age in arid areas of Africa , the Arabian Peninsula and the Middle East . The increased incidence of syphilis in Bosnia and Herzegovina was also referred to as endemic syphilis .
Pathogens

The pathogen, a gram-negative screw bacterium from the family Spirochaetaceae , was initially classified as a separate species ( T. endemica ) alongside the other pathogens causing treponematosis . However, the similarity to the causative agent of syphilis is so high that today both are classified as subspecies of the same species T. pallidum . The subspecies T. p. ssp. endemica of endemic syphilis, however , lacks the pathogenicity factors that T. p. ssp. pallidum and give it the ability to infect nerve tissue and to persist there. The subspecies can not be distinguished morphologically . The helical bacterium is 5 to 20 µm long and 0.1 to 0.4 µm wide; it can move around the longitudinal axis by rotating movements. It is very environmentally unstable and sensitive to dehydration, so it is only released through direct skin / mucous membrane contact or indirectly (but only promptly) through eating utensils, drinking vessels, etc. transferred.
Dissemination and transmission
Endemic syphilis is currently mainly to be found in nomadic population groups who live in a close social group and at the same time under poor hygienic conditions. It occurs among nomads in the Sahel region , among pygmies on the border between the Democratic Republic of the Congo and the Central African Republic, and Bedouin peoples of the Arabian Peninsula (Saudi Arabia) and the countries of the Middle East. In other dry, arid areas such as Iraq , Iran , Kazakhstan , Uzbekistan , Turkmenistan , Afghanistan and China ( Xinjiang ), a high prevalence was previously detectable, but the epidemic situation is currently unclear.
The disease is given different names in the respective areas, which in the medical literature were initially considered to be different diseases. In addition to the Bejel, which is used in German and English (from Arabic بجل Badschal , DMG Baǧal for syphilis) or Belesh, the African disease is also called Njovera. Further names are Dichuchwa, Frenga, Siti or Skerljevo. According to historical reports, the disease appears tohave occurredearlier in Ireland (as button scurvy ), Scotland ( sibbens ) and Norway ( radesyge ). Endemic syphilis also occurred in individual villages in Bosnia until before the Second World War .
Bejel is transmitted through close social contact, kissing, breastfeeding , skin-skin contact and indirectly through flies and when eating utensils and drinking vessels are shared directly. Patients with open skin lesions are particularly infectious.
Clinical picture

Like all treponematoses , Bejel also shows a multi-phase course. The primary lesion at the point of entry of the pathogen is usually not visible or is completely absent. After an incubation period of two weeks to three months, inflammation of the corners of the mouth ( stomatitis ), small lesions (plaques) on the oral mucosa and easily bleeding ulcers develop . The anogenital region and the larynx can also be affected. Skin changes or bone involvement rarely occur at this early stage. This first stage subsides again after six to nine months without impairing the general condition. Most infections now move into a latent stage in which long bones (typically the shin ) and facial bones (preferably the nasal bone ) become infected with proliferative, deforming periostitis . There are ulcerating skin lesions (gummata) and larger skin defects as in some forms of yaws . The infection can progress for years and lead to significantly disfiguring tissue defects. In contrast to true syphilis, Bejel never affects the central nervous system or the large vessels ( aortitis ) or the heart.
Diagnosis
The reliable diagnosis is made by microbiological evidence of the pathogen. T. pallidum can not be grown on artificial culture media and can only be stained with Gram stain with difficulty. Routine examination of tissue or exudate will usually not show the very thin bacteria. The pathogen can be detected by native dark field microscopy (mobile spirochetes) or specific fluorescence microscopy . In the early phase of the disease, antibodies can be detected, which, like in syphilis, can be detected using TPHA (Treponema pallidum hemagglutination assay) or FTA Abs test (fluorescence Treponema antibody absorption test). A differentiation between the subspecies is not possible in routine testing with commercial test systems; this is reserved for special laboratories.
Therapy and prophylaxis
Endemic syphilis is treated with antibiotics for at least two weeks with penicillin ; for mild illnesses in the early stages, a one-time depot preparation is sufficient. Resistance of the pathogen to penicillin has not yet been observed. If the patient is hypersensitive to penicillin, macrolides or tetracyclines are also given. In the case of a severe, widespread illness, drug treatment should be continued for longer. As with all treponemas, a Herxheimer reaction can occur one to two hours after the start of treatment due to massive breakdown of bacteria . Extensive tissue defects can only be covered or reconstructed by plastic surgery after adequate antibiosis .
There is no vaccine against treponema. The prophylaxis is limited to the prevention of transmission, on the one hand by improving sanitary conditions and education on the transmission path, the other by elimination of the pathogen from endangered populations through improved medical care.
swell
- W. Lang, Th. Löscher: Tropical medicine in clinic and practice. 3. Edition. Stuttgart 2000, ISBN 3-13-785803-8 , pp. 309f.
- JL Pace, GW Csonka: Endemic non-venereal syphilis (bejel) in Saudi Arabia. In: British Journal of Venereal Diseases (1984) 60 (5), pp. 293-297 PMID 6487985 , PMC 1046341 (free full text)
- JL Pace, GW Csonka: Late endemic syphilis: case report of bejel with gummatous laryngitis . In: Genitourinary Medicine (1988) 64 (3), pp. 202-204 PMID 3410469 , PMC 1194201 (free full text)
Individual evidence
- ↑ F. Kogoy: The endemic syphilis in Bosnia and Herzegovina. In: Dermatologica. Volume 79, 1939, pp. 361-369.
- ↑ RR Willcox: Njovera: An endemic syphilis of Southern Rhodesia. Comparison with bejel . In: The Lancet . (1951) 10; 1 (6654), pp. 558-560 PMID 14805127
Web links
- Tissue defects on the face after endemic syphilis
- Papules and ulcers in a child
- global.sbs.ohio-state.edu [1] Bejel proliferative periostitis (bone preparation)
{kind=link}
{kind=link}
{kind=link}
![[1]](http://global.sbs.ohio-state.edu/cd-contents/Ortner-slides/Book%20104-jpg/104-415.jpg){kind=link}