
Triple osteotomy

The triple pelvic osteotomy (syn. Triple pelvic osteotomy - DBO, Tönnis osteotomy, modified Tönnis osteotomy or triple pelvic osteotomy - TPO) of the pelvis is one of the most recent surgical techniques for the treatment of hip dysplasia (abbreviation HD) . The concept is explained by the bony transection ( osteotomy ) of all three (triple) the hip socket forming pelvic bones ( ischial , pubic bone and iliac ).
The aim of the operation is to improve the unfavorable biomechanical conditions in the hip joint that exist in hip dysplasia. The procedure promises success even if the hip joint wear is beginning and is already progressing ( coxarthrosis ), so that the need for a joint replacement ( endoprosthesis ) can be delayed or even avoided entirely.
In the triple osteotomy, the bony hip socket (acetabulum) is completely detached from the rest of the hip bone . This makes it possible to reconstruct the canopy of the femoral head three-dimensionally and almost anatomically. The surgical procedure - as it is used today - was first carried out in the mid-1970s by Dietrich Tönnis with the help of Klaus Kalchschmidt at the Dortmund City Clinic and developed there.
A technically comparable procedure that is carried out in veterinary medicine on young dogs with hip dysplasia is also often called triple pelvic osteotomy (TPO).
Anatomical peculiarities
- Pelvic anatomy
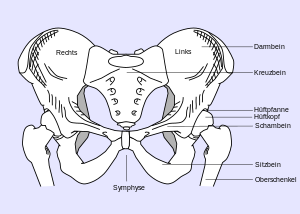
Healthy Pelvis Anatomy (Front View)
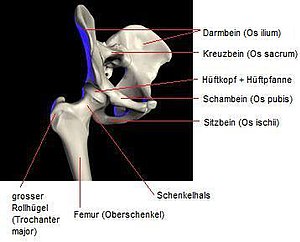
Model of a healthy pelvis


The pelvis is the center of the human body and unites the spine with the lower extremity (leg). At the same time, important organs such as B. the bladder, the rectum, the sexual organs and their appendages, directly in the pelvic vault. Large vessels and nerves ( sciatic nerve , pelvic artery and vein) fork here. After all, numerous muscles, tendons and ligaments attach to the pelvis, which are important for body statics and especially for the complex hip movements.
The vault-like structure of the pelvis and the sensitive soft tissue conditions (nerves, vessels, muscle-tendon attachments) make the access routes complicated.
The dysplastic cup
A hip dysplasia leads to minor growth of the joint and therefore to an inferior education of the bony roof of the femoral head. The lateral and ventral acetabular cavities are only partially or not at all, which leads to a decentering of the femoral head. Biomechanically, the insufficient roofing and the decentering of the head lead to a shift in the stress zones. The smaller the supporting surface (here the dysplastic socket), the higher the resulting load pressure (transmitted through the femoral head).

Healthy hip joint with a physiologically developed socket core

Dysplasia hip. Inadequate lateral and ventral roofing / acetabular cavity.

Biomechanics of the hip joint in normal position

Biomechanics of the hip joint in dysplasia

healthy pan hole

Pan orifice with dysplasia






Goal of the triple osteotomy
The aim of this operation is to turn and swivel the acetabulum (ie the hip socket) in all planes so that the femoral head is almost completely covered again, as if by a healthy socket ("containment") . That is why one speaks of a three-dimensional reconstruction. Since the malformation in hip dysplasia is not limited to the lateral acetabular cavity, but affects the entire acetabular hemisphere, it is not enough to improve the roofing in only one direction. The aim is to anatomically (as far as possible) reconstruct the dysplastic cup. This also includes the inclusion of the rear and especially the front canopy.
Depending on the severity of the disease and the resulting deformation of the femoral head and acetabulum, the reconstruction must also adapt to the given circumstances. Is the femoral head z. B. flattened or deformed in such a way that the lateral femoral neck-head junction is omitted, too far corrective pivoting of the socket can lead to restrictions in movement. A so-called femoro-acetabular impingement (FAI for short) occurs. In these cases, the reconstruction - i.e. pivoting the cup - is only carried out “as far as possible”. Sometimes remodeling measures are also necessary on the femoral neck or on the edge of the head.
In the case of hip dysplasia or Perthes-related femoral neck anomaly (see CCD angle ) that prevent or limit anatomical reconstruction, an additional intertrochanteric osteotomy can be performed. Most hip dysplasias lead to a coxa valga and often to a coxa antetorta due to the elevated position of the femoral head . Accordingly, if necessary, a derotation varization osteotomy (DVO, see Osteotomy ) is performed.
Indications and contraindications
Indications for a triple osteotomy are congenital hip dysplasia of the adult pelvis and secondary hip dysplasias, for example in the context of neurological diseases such as infantile cerebral palsy or poliomyelitis . Dysplasia coxarthrosis (incipient joint wear of the hip with existing hip dysplasia) is also an indication - especially in the early stages - as is Perthes disease (early childhood necrosis of the femoral head) with severe flattening of the femoral head. Rare forms of femoro-acetabular impingement , for example in the case of a protrusion acetabuli (congenital malformation with too deep acetabular vault) , are also an indication for triple osteotomy.
Age factor
The triple osteotomy is not the universal procedure for every patient with hip dysplasia or patients of any age. It is desirable, but not mandatory, to perform this procedure only after all growth zones have been completely closed. However, in growing children, triple osteotomies have also had good results and have not stunted growth.
There are different views as to the age at which such an operation can be performed. At times, children from the age of seven were also treated with this procedure. At this age, however, simpler and gentler surgical techniques, e.g. B. the acetabuloplasty achieved the same results. In most cases, the complete closure of the growth plates on the pelvis is achieved between twelve and 14 years of age, which according to experts should also be considered the lower limit of the therapy age.
The upper age limits are much more difficult to set. If there are no contraindications , patients can still be treated with this operation at the age of 50. The degree of joint wear and the general physical condition of the person are decisive for this. When establishing the indication, it is also important to ensure that it is a serious and physically stressful operation that involves strenuous and long rehabilitation, but can save the patient a hip prosthesis under certain circumstances.
Absolute contraindications
Absolute contraindications are advanced dysplasia coxarthrosis with a corresponding restriction of movement, diseases or secondary conditions of the muscle-tendon apparatus of the hip that would make the three-dimensional pivoting of the acetabulum impossible, inability to undergo anesthesia or surgery for other medical reasons, pregnancy , bacterial-inflammatory changes in the area the pelvic bones (e.g. osteomyelitis or bacterial arthritis of the hip joint), wound healing disorders, inflammatory changes in the surgical field, and tumors or metastases in the pelvic area.
Diagnosis

Conventional x-ray images of the pelvis, so-called pelvic overview images , are made both for the precise assessment of the hip dysplasia and its severity and for planning the operation .
Computed tomography (CT) or magnetic resonance imaging (MRI) are only necessary in exceptional cases, for B. to be able to better assess the degree of joint damage. Computer methods for the three-dimensional representation of organs have not become established in the pelvic area. However, 3D-CT of the pelvis is used in CT-based navigation methods (see below).
Operational sequence
Anesthesia and pain therapy
Since this procedure leads to severe pain postoperatively, an epidural catheter is usually placed, which is used to treat pain for several days after the operation. Typically this is done in the surgery department or in an anesthesia preparation area shortly before the actual anesthesia. The operation is performed under general anesthesia with intubation and ventilation .
storage
The three different approaches make it necessary for the patient to be positioned on their side or on their stomach for the first step - the transection ( osteotomy ) of the ischium. Positioning on the opposite side has now become established, as it allows the patient to be turned on their back in a sterile manner, i.e. without new disinfection and covering. For the second and third access ( pubic and iliac bone ) the patient remains in the supine position.

Surgical technique
In the first step, the ischium is cut. The ischium is cut at an angle to its course and remains without osteosynthesis (surgical reassembly). After the patient has been turned onto his back, the pubic bone osteotomy is performed. Before attempting the osteotomy of the iliac bone, the surgeon screws in a guide screw above the socket. Using this stable screw, he can turn and swivel the socket fragment under X-ray control until the socket has reached the desired position ( joystick technique). The iliac bone is then attached to the socket fragment by osteosynthesis with screws or wires. An osteosynthesis of the pubic bone is not mandatory, but it does contribute significantly to the overall stability.

Heavy HD left> right before the operation

after the operation
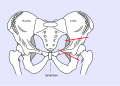
Sketch of the hip dysplasia left. with drawn osteotomy lines

Sketch of the finished triple osteotomy (dashed red: route of the pelvic screws for fixation)




Complications
Unexpected surgical results are also seen as complications. A triple osteotomy can lead to changes in leg length, incorrect corrections and faulty osteosynthesis. Postoperative persistence of the symptoms is also seen as a complication. As with any other operation, the success of the treatment cannot be guaranteed.
General intraoperative complications
As with any operation, bleeding or organ injuries can also occur here, so an autotransfusion system is usually used . If there are no complications, a blood loss of less than one liter is to be expected.
Special intraoperative complications
Injuries to the hip joint itself are extremely rare and should not be considered a complication. Fractures in the pelvic area due to osteotomies or screw connections can occur and are treated directly during the operation. Occasionally, the dissection of the pubic bone results in irritation or injury to the lateral cutaneous femoral nerve . As a result, permanent or reversible sensitivity disorders occur in the area of the outer leg and groin. In men, there is a risk of injuring the spermatic cord or the parallel vessels and nerves. The preparation for the ischial bone runs very close to the sciatic nerve , which can be injured in the process. Injury to the femoral vein can occur during pubic bone dissection ; injuries to the femoral artery have not been described.
Post-operative complications
Typical early complications after bone surgery, such as failure of the osteosynthesis materials (screws or wires) and screws breaking out of the bone, are rare. As with any bone operation, bone necrosis or bone healing disorders can also occur here . General surgical complications are e.g. B. wound healing disorders , thromboses / embolisms , other coagulation disorders and wound infections .
Late infections, caused by a spreading focus of inflammation in the body, are described as extremely rare. In operations near the joint, it can u. There may be postoperative mobility restrictions. Pubic bone pseudarthrosis is a real late complication . The two fragments of the pubic bone do not grow together as bones, but rather as connective tissue. This pseudarthrosis must be revised in any case, i.e. operated again, as otherwise sufficient stability in the pelvis will not be achieved.
Follow-up treatment and rehabilitation
In the first four to six weeks, the focus of follow-up treatment is on mobilizing the patient and, if necessary, on pain therapy . The leg on the affected side must not be subjected to any or very little weight during this time. The patients have to learn to walk with crutches or other walking aids. Furthermore, the patient exercises under physiotherapeutic guidance how to sit and stand up. In the following weeks, the load on the affected leg is slowly and steadily built up in an inpatient or outpatient follow- up treatment, not least to strengthen the muscles. Climbing stairs and other everyday movements must also be rehearsed in the time it takes to achieve full resilience. To check the healing process of the bones, further x-rays of the pelvis are taken at regular intervals. The duration and the detailed procedure of the follow-up treatment vary depending on the surgeon and individual factors.
After discharge from the follow- up treatment, the patients are generally accompanied by physiotherapy for some time. Furthermore, there is the possibility of rehabilitation aftercare programs of the pension insurance, such as B. IRENA ( intensified rehabilitation aftercare ) or ASP to continue to receive care .
The osteosynthesis materials are removed after about a year.
Success rates

As has been shown in recent years, three-dimensional acetabular reconstruction procedures - such as the triple osteotomy according to Tönnis - offer many possibilities. The most important of these is surely to save a hip joint from wear and tear caused by dysplasia. Nevertheless, the success of this operation stands and falls with many influencing factors, not least with the patient himself.
Influencing factors that negatively influence or complicate the postoperative course are e.g. B. Obesity, smoking and poorly trained ("flaccid") muscles. Excessive obesity (overweight) stresses the osteotomies and osteosynthesis just as it stresses the joints of the lower extremities. This is particularly important in the first few weeks, when the operated pelvis may only be partially loaded. It has been proven that smokers have a “softer”, osteogenically less potent bone substance than non-smokers. The ossification , that is the (re) formation of bone is significantly influenced by the train the muscles to the bone. The stronger the muscles, the greater the tension on the bones during tension.
The earlier hip dysplasia is detected, the easier and more effective the therapy. As long as the joint does not show any arthritic changes, the chances of a prosthesis-free life are very high. When wear and tear begins, it is quite possible to postpone the need for an endoprosthesis for ten to 15 years or even longer.
There are already individual studies on medium-term results with regard to the triple osteotomy. The studies consistently look at patients with hip dysplasia . The age range of the studies averages between 13 and 46 years. All were operated on using the Tönnis technique and re-examined in an identical manner. The follow-up period for the study from 2002 is 11.5 years, making it the longest-term study. Here 46 women and eight men with - until then untreated - hip dysplasia were examined, all of whom had been operated on using the Tönnis technique. The development of coxarthrosis could be prevented in over 90% of the patients during the duration of the study. One patient had to be fitted with a hip replacement 11 years after the Tönnis osteotomy . During the follow-up examination, almost 90% of the patients reported a clear improvement in their symptoms with reduced pain and increased mobility compared to the time before the triple osteotomy. Approx. 85% of the examined patients assessed the result of the operation subjectively as "very good".
history
Since the 1950s, the Chiari displacement osteotomy, mostly in conjunction with an intertrochanteric varus osteotomy, has been the most common operation for treating hip dysplasia in the closed pelvis. Soon intertrochanteric OT was abandoned more and more frequently , as it was found that the optimal therapy was to be found in the anatomical reconstruction of the acetabulum. Since with the Chiari method the reconstruction only takes place in one plane, this was in most cases - for an anatomical reconstruction - insufficient.
In the 1960s, numerous surgical techniques were developed in which the acetabulum - in various ways - could be detached from the pelvic continuity and pivoted. In 1962, the Blavier brothers tried out such a technique for the first time, in which the cup was spherically detached and re-attached in a corrected position. In 1965 Wagner performed a similar operation. Numerous modifications of this spherical pelvic osteotomy followed (Eppwright, Tagawa, Ganz, etc.), which is still used today (mainly in the United States and Switzerland).
The first triple osteotomy was described by LeCoeur in 1965. Several surgeons emulated him and developed variations of the triple osteotomy. Steel developed another shape in 1972 that has remained to this day. The posterior (rear) access to the ischium is not used here, which is a cosmetic advantage. The disadvantage of this method is that the sciatic nerve cannot be exposed during the steel osteotomy. Tönnis and Kalchschmidt joined them in 1976 with the triple osteotomy described here. They placed the osteotomy planes and thus the pivot point a little closer to the socket and osteotomized the ischium via the posterior approach described. Both procedures are the ones typically used today.
The first operations - using the Tönnis technique - took between six and ten hours in the 1970s and presented a number of problems and complications. Today, the normal operation time is two to four hours. Experience over the past few years has made the access routes, the technique of swiveling the cup and osteosynthesis easier and safer. Today, the triple osteotomy is a standard procedure for treating hip dysplasia and is carried out in numerous clinics.
Computer-assisted triple osteotomy
Since the mid-1980s, computer systems have been developed that are intended to serve as “pointers” for the surgeon during certain interventions. The term “computer-assisted surgery” (CAS) has become indispensable in many areas of surgery, but especially in bone surgery. Numerous, technically more precise systems are constantly coming onto the market. The first so-called OR navigation systems were used in neurosurgery for micro-operations on the brain. The "Navigated Triple Osteotomy" has been meticulously worked on since 1996. Procedures that are already in regular use require prior computed tomography to calculate a 3D image of the pelvis. In this way, the navigation system can instruct the surgeon using special instruments, which are visible for navigation, both for saw cuts and for swiveling the socket. This is just one example of the various technical options. The techniques as well as the instruments and devices are becoming increasingly easier and faster. Studies on the success of navigation in pelvic osteotomies are already available.
Triple osteotomy in dogs
In veterinary medicine, triple osteotomies have so far only been performed on dogs with hip dysplasia . Since the operation is complex, a precise cost-benefit analysis is necessary. A triple osteotomy is only indicated in young dogs that are intended to be used as a working dog. The prerequisite is that no or only minor osteoarthritis changes in the hip joint can be detected radiologically, the reduction angle in the hip joint is less than 30 ° and the subluxation angle is less than 10 °. The reduction angle is understood to mean the angle at which the head of the thigh bone jumps back into the acetabulum when the limb is spread apart ( abduction ). The angle of subluxation is defined as the angle at which the head of the femur jumps out of the socket during inward movement ( adduction ).
The triple pelvic osteotomy is mainly performed using the Slocum & Slocum method, whereby after the three pelvic bones have been severed, the acetabulum is rotated and displaced outwards. The subsequent fixation of the pelvic bones is done with specially made plates.
See also
Literature and Sources
- Breusch, Mau, Sabo: Clinical Guide Orthopedics . Elsevier 2006, ISBN 9783437224713 .
- Klaus Buckup , LC Linke, W. Cordier: Pediatric Orthopedics . Thieme 2001, ISBN 3136976029 .
- V. Bühren, O. Trentz, U. Heim: Checklist traumatology . Thieme 2005, ISBN 978-3135981062 .
- J. Duparc: Surgical Techniques in Orthopedics and Traumatology. Pelvic ring and hip . Elsevier 2005, ISBN 3437225561 .
- AB Imhoff, R. Baumgartner: Checklist Orthopedics . Thieme 2006, ISBN 3131422815
- Ann L. Johnson and Donald A. Hulse: Diseases of the joints . In: Theresa Welch Fossum (Ed.): Small Animal Surgery . 2nd Edition. Mosby, 2002, pp. 1023-1157.
- W. Konermann: Navigation and Robotic in Joint and Spine Surgery . Springer, 2003, ISBN 3540433058 .
- R.-P. Meyer, A. Gächter: Hip surgery in practice . Springer, 2005, ISBN 978-3540227182 .
Individual evidence
- ↑ a b c R. Graf: The hip joint. From babies to endoprostheses . In: Journal for Mineral Metabolism . Volume 11, Issue 1, 2004, pp. 12-21 www.kup.at/2004 11-1
- ↑ a b c C.J. Wirth: Orthopedics and orthopedic surgery. Bd. Pelvis / hip . Thieme 2004
- ↑ a b Angela Ruwell: Individual templates for triple osteotomy . dissertation
- ↑ a b c d e f g h i Axel Küpper: Medium-term results of the triple pelvic osteotomy according to Tönnis . Dissertation (full text)
- ^ A b c d e Meyer, Gächtler: Hip surgery in practice . Springer 2005.
- ↑ a b c d e J. Duparc: Surgical Techniques in Orthopedics and Trauma Surgery . Bd. Pelvic ring and hip. Elsevier 2005
- ↑ a b c A. B. Imhof, R. Baumgartner: Checklist Orthopedics . Chapter Pediatric Orthopedics. Thieme 2006.
- ^ J. Duparc: Surgical Techniques in Orthopedics and Trauma Surgery . Bd. Pelvic ring and hip. Elsevier 2005. Summary of Surgical Technique Triple Pelvic Osteotomy
- ↑ JM Hoogendoorn, RKJ Simmermacher: Smoking is detrimental to the healing of bones and soft tissues . In: The trauma surgeon . Volume 105, No. 1 / January 2002. Springer.
- ↑ ME Müller, M. Allgöwer: Manual of osteosynthesis. AO technology . Chapter bone healing. Springer 1992.
- ↑ D. Tönnis, K. Kalchschmidt, A. Heineke: The pivoting of the acetabulum by triple osteotomy of the pelvis. Significance and indication in the variety of surgical corrections of the dysplasia hip . In: Orthopedic Practice . Volume 35, pp. 607-620.
- ^ K. Chiari: Results with the pelvic osteotomy as acetabular surgery . In: Journal for orthopedics and their border areas . Volume 87, 1955, pp. 14-26.
- ↑ L. Blavier, J. Blavier: Traitement de la subluxation de la hanche . In: Rev-Chir-Orthop . Volume 48, 1962, pp. 208-213
- ^ H. Wagner: Osteotomies for congenital hip dislocation . In: The hip. Proceedings of the fourth open scientific meeting of the Hip Society . St. Louis 1976, pp. 45-66
- ↑ M. Leuning, R. Ganz: Berner periacetabular osteotomy . In: Orthopedist . Volume 27, 1988. pp. 743-750.
- ^ P. Le Coeur: Correction des défauts d'orientation de l'isthme iliaque . In: Rev-Chir-Orthop . Volume 51, 1965, pp. 211-212
- ↑ D. Tönnis: A new form of pivoting the acetabulum using a triple osteotomy to enable subsequent hip prosthesis treatment . In: Orthopedic Practice . Volume 12, 1979, pp. 1003-1005.
- ↑ H.-W. Staudte, E. Schkomodau: Pelvic osteotomy with the DISOS template navigation . In: W. Konermann: Navigation and Robotic in Joint and Spinal Surgery . Springer 2003, ISBN 3540433058 .
- ^ B. Slocum and TD Slocum: Pelvic osteotomy for axial rotation of the acetabulum segment in dogs with hip dysplasia . In: The veterinary clinics of North America. Small animal practice . Volume 22, 1992, p. 645.