
Field of view (perception)
With visual field is called in physiology , ophthalmology , neurology and general of perception research , the field of view of the eye to its natural, anatomical site, weighted with the sensitivity of the central nervous system that receives the light pulses and evaluates. The field of vision represents both the space that is visible to an immobile eye (in a 2-dimensional sense) and "... the entirety of the optical-sensory stimuli that [...] are directed to the cerebral cortex and perceived."
A distinction is made between the monocular visual field of the right and left eye alone, from the binocular visual field, which is the sum of the two monocular visual fields. In humans, the fields of vision of both eyes overlap in certain areas. In binocular field deck one finds fusion instead of the right and left eye into a single of the two images. The so-called horopter is a prerequisite for the development of spatial vision . In an adult, the horizontal extension of the binocular field of view is about 214 ° (± 107 ° on each side), the vertical about 60 ° -70 ° upwards and 70 ° -80 ° downwards. The binocular field of view extends over about 1/3 of the entire space.
The field of vision represents the entire area in which (without the aid of eye movements) visual perception is possible. Clear recognition, however, is only possible within the central area of the fovea ; the quality of perception in terms of visual acuity , pattern recognition and color vision decreases the more peripheral the visual stimuli are. The sensitivity for moving objects also decreases peripherally, but less so than other visual functions, so that in peripheral vision there is a relative superiority of motion vision . The periphery of the visual field is therefore particularly important for recognizing dangerous situations. The twilight vision has, if one looks an optimum at about 20 ° eccentricity, which is why weak shining stars looks best on them slightly over.
The quantitative, functional testing and measurement of the visual field is called perimetry . This examination is not only of great importance for diseases of the visual system , but can also be part of a general neurological diagnosis.
Representation of the field of view


The data obtained with the help of perimetry are usually displayed in two dimensions on a sheet of paper or a screen. The measured values obtained on a hemispherical surface are projected onto a flat surface in the form of an azimuthal image . In the center lies the point of sharpest vision ( fovea ); the radial lines emanating from it are the meridians . The above-mentioned expansion of the field of vision (“horizontal, vertical upwards, downwards”) relates to the distances from the horizontal or vertical meridian. In the figure, the blind spot can be seen as a black oval at approx. 18 ° to the right (for the right eye).
The visual field of each eye represented in this way typically has the shape of a horizontal oval, usually with a flat, inferonasal indentation. The projection causes a reduction in size. So the field of view appears much narrower in two-dimensional representation than it is in reality.
In classical kinetic perimetry, the sensitivity of the CNS is represented by lines of equal sensitivity, so-called isopters. These are determined with the help of (slowly) centripetally moving stimulus marks of decreasing size and intensity .
Static perimetry uses stationary stimulus marks of increasing or decreasing intensity. The graph shows the location and the intensity of the weakest stimuli that were just perceived ( perception threshold ).
Limitations and Defects
Limitations of the visual field are called visual field defects . They can be caused by damage to the retina of the eye, the visual pathway , or the cerebral cortex . The latter are known as cerebral visual field defects. Divided according to the location and size of the damage in the visual field, a distinction is made between hemisphere blindness , quadrant anopsias and scotomas . If the damage lies in the eye or the optic nerve, the visual fields of the two eyes are usually affected differently ( heteronymous damage ). If, on the other hand, the location of the damage is in the visual pathway after the optic nerve junction , the visual fields of both eyes are affected in the same way ( homonymous damage ). The reason for this is that due to the partial crossing of the optic nerve fibers in the optic nerve junction, the left (or right) visual field of both eyes is further processed in the same, opposite (right or left) hemisphere. In the case of half-sided blindness, z. B., regardless of the eye, the left (or the right) visual field affected. The cause of this damage is often a stroke or head trauma , and less often a tumor.
Smaller restrictions of the visual field are called scotomas . They can appear anywhere in the field of vision (called central scotomas occurring in the center) and have different sizes. They are classified as relative (decreased but not abolished visual sensitivity) or absolute (lack of any visual sensitivity) , depending on the extent of the loss of sensitivity . The same classification applies to scotomas according to the location of the damage (eye, visual pathway, cerebral cortex); an example of damage to the eye is Bjerrum's scotoma in glaucoma .
Scotomas are further subdivided into consciously perceived, positive scotomas, or pseudoscotomas and unconsciously present, negative or real scotomas. Positive scotomas in the sense of the above definition are z. B. caused by glasses, the nose , eyebrows and cheekbones , the eyelids ( ptosis ) and opacities of the optics of the eye (cornea, lens, vitreous humor). Fresh retinal disease can cause a consciously perceived scotoma. The ciliated scotoma is also a positive scotoma originating in the central nervous system. An absolute, but not pathological, negative scotoma is the so-called blind spot , which represents the point on the fundus at which the optic nerve emerges from the eye.
Concentric visual field deficits up to the so-called tube visual field or tunnel vision can arise not only from diseases of the retina ( retinopathia pigmentosa ) and the optic nerve but also, for example, as a result of excessive alcohol consumption, medication or psychological disposition ( simulation ).
Other visual field terms
The intactness of the visual field in the sense of the usual (light) perimetry is neither a necessary nor a sufficient condition for seeing in the corresponding visual field area. On the one hand, moving stimuli are perceived much better in the peripheral field of vision than the static or slowly moving stimuli used in perimetry. On the other hand, the intactness of a visual field area in the sense of standard perimetry says nothing about whether more complex stimuli are perceived. In practical applications, other visual field terms have therefore also proven useful. The useful field of view in diagnostics for driving fitness has become known. The shape recognition field of view says something about whether simple shapes (such as characters, traffic signs) are recognized in the corresponding field of view area.
In addition to standard perimetry, other perimetric methods are also used in ophthalmological diagnostics, such as B. the flicker perimetry according to Frisén, Rauschfeldkampimetrie according to Aulhorn, u. a.
Visual field of animals

Dove: Prominent eyes on the side of the head

Owl: Deep set eyes on the front of the head



The visual field of other living beings differs from that of humans in part quite clearly:
- Frog about 330 °
- Flying approx. 300 ° ( compound eyes )
- Kestrel 300 °
- Crocodile 290 °
- Barn owl 160 °
- Snails (bowl and hole eyes) about 100 ° to 200 °
- Jellyfish and worms (flat eyes) 100 ° to 180 °, with several eyes - taken together - larger.
The simple eyes (pit, flat and point eyes ) as well as bowl and hole eyes are not imaging, but only give approximate directions . Real images are created by the compound eyes of higher insects through the grouping of elongated light channels , as well as the lens eyes of larger animals. Escape animals such as horses or rabbits have their eyes on the side of their heads and can see a large section of the room without moving their heads, while predators such as cats have their eyes close together and in front of them and thus have large cover areas with good spatial resolution.
Field of view of horses

Horse eye
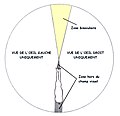
Horizontal field of vision
gray: blind spot
yellow: binocular area
white: monocular area
The horse can focus binocularly on distant objects by lifting its head.

When the head is upright, the binocular focus is close to his legs.




Horses have very large eyes that sit on the sides of the head. The horizontal field of view of horses is approximately 350 °. Despite the wide field of view, you cannot see back without moving your head. You avoid stepping on horses from behind so as not to frighten them. There is also a blind spot right in front of the horse's head. The spatial vision is narrow to a comparatively, about 65 ° wide, restricted area before the horse. A horse can only assess obstacles in this area, for example . In the remaining 285 ° the horse can only see with one eye at a time. The vertical field of view is comparatively limited upwards. This is why horses lift their heads when they want to focus on distant objects, for example when assessing an obstacle while jumping . They lower it when looking at objects in front of their legs, for example when grazing .
Demarcation
From the field of view which is used for the visual perception of visual stimuli in the outdoor space that is vision to distinguish in its various forms. This is based on a targeted fixation with the help of eye movements and in this respect relates purely to the oculomotor system.
Web links
- Sk2 guideline for visual perception disorders of the AWMF , status 04-2017. PDF accessed on January 26, 2018
On the history of the concept of the field of vision and perimetry
literature
- Herbert Schober: Seeing. Volume 1. 2., improved and expanded edition. Fachbuchverlag, Leipzig 1957.
- Gottfried Gerstbach : Eye and sight - the long way to digital recognition. In: The Star Messenger. Issue 8, 2000, ISSN 0039-1271 , pp. 160-180.
- Inge Flehmig: Normal development of babies and their deviations. Early detection and treatment. 5th, unchanged edition. Thieme, Stuttgart a. a. 1996, ISBN 3-13-560605-8 .
Individual evidence
- ↑ a b Robert F. Schmidt, Gerhard Thews (Ed.): Physiologie des Menschen , 21st corrected edition, Springer Verlag, Berlin a. a. 1983, ISBN 3-540-12222-2 .
- ↑ Space is meant here in a two-dimensional sense, as a spherical surface around the observer. The field of view does not represent the depth of the surrounding space as perceived by means of stereo vision .
- ↑ a b c d Strasburger, H. (2003). Indirect vision. Shape recognition in the central and peripheral visual field. Göttingen: Hogrefe
- ↑ a b Theodor Axenfeld (founder), Hans Pau (ed.): Textbook and atlas of ophthalmology. 12th, completely revised edition. With the collaboration of Rudolf Sachsenweger a . a. Gustav Fischer, Stuttgart a. a. 1980, ISBN 3-437-00255-4 .
- ↑ a b In most textbooks, the horizontal diameter of the field of view is incorrectly stated to be too small, namely only 180 °. The reason for this is, on the one hand, the technical limitation of modern commercially available spherical perimeters , the measuring range of which only extends to 180 ° or even less. At the same time, the standardized stimuli used are not visible outside 90 °. Another reason is probably the false assumption that light rays that hit the side at an angle of 90 ° (i.e. tangentially) cannot reach the eye at all. In fact, however, they can even hit the cornea laterally at angles slightly larger than 90 ° and still be directed into the eye by its refractive power.
- ↑ a b Traquair's illustration showing the size of the field of view
- ^ Mathur, Gehrmann, Atchison (2013). Pupil shape as viewed along the horizontal visual field . Journal of Vision 13 (6): 3 1-8.
- ↑ Henning Rönne: On the theory and technique of Bjerrrum's visual field examination . In: Archives for Ophthalmology . 78, No. 4, 1915, pp. 284-301.
- ^ Harry Moss Traquair: An Introduction to Clinical Perimetry, Chpt. 1 . Henry Kimpton, London 1938, pp. 4-5.
- ↑ a b Similar limits were already reported in the 19th century by Alexander Hueck (1840, p. 84): “I found a circumference of 110 ° outwards from the visual axis, only 70 ° inwards, 95 ° downwards, upwards 85 °. So when we look into the distance, we overlook 220 ° of the horizon. ”From: Hueck, A. (1840). From the limits of sight. Archives of Anatomy, Physiology, and Scientific Medicin, 82-97.
- ^ Robert H. Spector: Clinical Methods: The History, Physical, and Laboratory Examinations. 3rd edition. 1990.
- ^ A b c H. Strasburger, I. Rentschler, M. Jüttner: Peripheral vision and pattern recognition: a review . In: Journal of Vision . 11, No. 5, 2011, pp. 1-82. doi : 10.1167 / 11.5.13 .
- ↑ Claus-W. Wallesch (Ed.): Neurology. (Diagnostics and therapy in clinic and practice). Elsevier, Urban & Fischer, Munich a. a. 2005, ISBN 3-437-23390-4 .
- ↑ M. Bruce Shields, Günter K. Krieglstein: Glaucoma: Basics of differential diagnosis therapy . Springer-Verlag, 2013, ISBN 978-3-642-77053-1 ( books.google.com ).
- ↑ Th. Axenfeld, H. Pau: Textbook of Ophthalmology , 13th edition, Gustav Fischer Verlag Stuttgart Jena New York 1992, ISBN 3-437-00504-9 , p. 51.
- ^ Frederick H. Roy: Ophthalmologische Differentialdiagnostik , Georg Thieme Verlag Stuttgart 1997, ISBN 3-13-108881-8
- ↑ Newsletter Uni Tübingen current No. 1/2011: Research
- ^ Rudolf Sachsenweger: Neuroophthalmology. Thieme Verlag, Stuttgart, 3rd edition, 1983. pp. 142 ff. ISBN 978-3-13-531003-9
- ↑ Torsten Schlote, Ulrich Kellner: Undesired drug effects in ophthalmology . Georg Thieme Verlag 2011, p. 99. ISBN 978-3-13-165141-9
- ↑ Th. Axenfeld (original), H. Pau (ed.): Textbook and atlas of ophthalmology . With the collaboration of R. Sachsenweger u. a., Stuttgart: Gustav Fischer Verlag, 1980. P. 50 ff. ISBN 3-437-00255-4
- ↑ This is also known as statokinetic dissociation .
- ↑ Dannheim, F. Flicker and conventional perimetry compared to structural changes in glaucoma. Ophthalmologist (2013) 110: 131. doi: 10.1007 / s00347-012-2692-y
- ^ Miller, Robert W. Western Horse Behavior and Training. Main Street Books, 1975. ISBN 0-385-08181-2 , ISBN 978-0-385-08181-8
- ↑ Hartley, C; Grundon, RA (2016). Chapter 5: Diseases and surgery of the globe and orbit. In Gilger, BC (ed.). Equine Ophthalmology (3rd ed.). John Wiley & Sons. p. 151. ISBN 978-1-119-04774-2 .
- ↑ Herbert Kaufmann (Ed.): Strabismus. 3rd, fundamentally revised and expanded edition. With contributions by Wilfried de Decker u. a. Georg Thieme, Stuttgart a. a. 2004, ISBN 3-13-129723-9 .
{kind=link}