
Tape bandage

A Tape Association ( English tape , tape ') of paving tape , often abbreviated as tape or taping referred, in sports medicine , trauma surgery and orthopedics both for treatment and for preventionused. It does not completely immobilize the treated joints or muscles, but only prevents unwanted or excessive movements (functional bandage). The effect is based on the fact that the plaster strips adhering to the skin transfer the forces that occur to the skin and thus support the capsule-ligament apparatus of a joint ( augmentation ) and improve the perception of body movement ( proprioception ). They can also counteract any swelling of the tissue ( compression ) or fix injured joints or bones to uninjured ones ( splinting ). The application possibilities of tape bandages are versatile, suitable bandages are described for all joints on arms and legs.
Basically, the plaster strips used for tape bandages are inelastic and coated on one side with an adhesive. Depending on the function, a distinction is made between anchor, rein, fixation and formwork strips. Bandage material that is applied to the skin as the first layer before the plaster strips are applied is called undersealing tape . Underlay tape and adhesive plaster strips are applied without any significant pressure. The prerequisite for this are both a competent diagnosis and appropriate specialist knowledge of the practitioner. Typical complications are skin irritation, compartment syndrome and premature loss of the stabilizing effect. The study situation for this form of therapy is inconsistent, depending on the indication and localization. For example, tape bandages are considered to be " [...] the best scientifically investigated external stabilization aid of the ankle ", but only one study of poor quality has been found for use in the case of a certain type of fracture on the fifth metacarpal bone.
The use of the English term tape in this context goes back to the 19th century. As early as 1892, Paul Carl Beiersdorf launched self-adhesive plaster strips under the name Leukoplast , which quickly led to new recommendations for associations.
Working principles
Tape bandages are functional bandages . Unlike plaster casts , they do not completely immobilize a joint , but allow a certain movement and thus function. In contrast to the orthosis , their effect is not primarily based on the stability of the material used, but is created through targeted application, with the adhesive tape strips used usually sticking firmly to the skin. The principles of action of tape dressings have not yet been conclusively clarified; a basic distinction is made between compression , splinting and augmentation and a positive proprioceptive effect (joints).
- Principle of augmentation
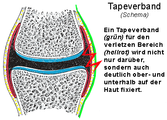
Positioning of the tape bandage (green).
Cartilage (blue), capsule (red), ligament (yellow), bone (gray).
Single tape rein


Augmentation - proprioception
In contrast to other dressings used in medicine, tape dressings can specifically augment (strengthen) the holding function of the capsule-ligament apparatus of a joint . For this purpose, inelastic strips of adhesive plaster are applied to the skin according to the course and function of injured or potentially endangered band structures . Tensile forces acting on the ligaments are thus transferred to the skin via the plaster strips . In addition to the purely mechanical effect, the proprioception improved by the tape bandage also plays an important role in stabilization. Athletes perceive unwanted movements better and can avoid them more easily. These two effects have been known for decades and lead to the fact that overstretching or renewed distractions of already injured ligaments (up to and including dislocations ) can be prevented.
In contrast to a plaster cast, however, the tape bandage does not lead to a complete abolition of mobility (immobilization) and thus also does not lead to the consequential damage associated with prolonged treatment. The tape bandage thus allows the mobility of a joint within suitable limits, but prevents harmful movements that go beyond these limits (functional bandage) . Stability and the degree of restriction of movement caused by a tape dressing depend on the material used and the method of application.
compression
Plaster strips can also be used as compression bandages . When applied to the arms or legs, their effect is comparable to that of (inelastic) zinc glue bandages , the permanent pressure of which is minimal during physical inactivity ( pressure at rest ), but the bandage opposes the expansion of the muscles during contraction (working pressure). If, in addition, elastic bandages are used for taping, the properties of such a tape bandage are similar to those of a conventional compression bandage with, depending on the elasticity of the materials used, higher resting and lower working pressure.
The application of a tape bandage as a compression bandage is also indicated as an immediate measure after injuries (within the meaning of the PECH rule ). Here, the inelastic material prevents unnecessarily strong swelling caused by an accident. Such a bandage applied as part of first aid should, however, be tight and should not be left for longer than an hour.
The application as a compression bandage is not specific for the tape bandage, there is no significant transfer of force to the skin. It is therefore not necessary to achieve an adhesive effect of the plaster strips on the skin that is comparable to that of the augmentation.

Splint
By applying a suitable bandage, certain types of bone fractures and ligament injuries can also be treated. These include, for example, unshifted fractures of the metatarsals and toes. The tape bandage is applied to the metatarsus so that the fractured bone is stabilized (splinted) by the four uninjured metatarsal bones. A broken toe is stabilized by fixing it to an adjacent toe with adhesive plaster and at the same time significantly reducing mobility in the base, middle and end joints ( plaster rein bandage ). Simple finger fractures can also be treated in a very similar way. For this type of splinting of an injured finger (or toe), the term buddy taping can be found in the Anglo-American literature .
These tape dressings must adhere very well to avoid shifting. However, the transfer of tensile forces to the skin plays a subordinate role. The stability of the dressing as such (its rigidity and the fixation of the injured to the uninjured bone) is essential for the effect . The most prominent example was the American athletic trainer and physiotherapist "Ducky" Drake, who did not tell his protégé CK Young at the 1960 Olympic Games in Rome that he had a fatigue fracture in the metatarsus that he taped for weeks. Young won the silver medal in the decathlon and only found out about his injury afterwards. Olympic champion Rafer Johnson was also one of Drake's trained athletes at UCLA .
method

The aim when applying a tape bandage is to restrict the range of motion of a joint only as much as necessary, but at the same time to stabilize its capsule-band apparatus in such a way that harmful extreme movements are avoided. The basic prerequisites for this are an exact diagnosis , a sufficiently good condition of the skin in the area of the planned bandage and the corresponding professional competence of the person applying it.
material
Inelastic, self-adhesive plaster strips , so-called tapes , are used to apply a tape bandage . Other dressing materials can also be used in addition.

It is essential that the adhesive tape irritates the skin as little as possible, but at the same time adheres well to it even when it is wet (sweat, rain) and that its properties remain sufficiently stable. Since a complete closure of the sweat glands is not possible when applying a tape, the material must also be permeable to water. Otherwise the tape dressing would quickly lose the necessary adhesion because it would be lifted off the skin over a large area by the sweat .
Patch sprays can reduce perspiration , but not prevent it. If they consist of a well-tolerated adhesive, they can reduce skin irritation from the tape bandage.
In order to reduce skin irritation in sensitive patients, strongly adhesive bandages coated with well-tolerated, low- allergenic (hypoallergenic) adhesives can be applied directly to the skin as the first layer ("underseal tape"). A tape bandage can then be applied in the usual way on this first layer.
In the case of tape dressings whose primary goal is not augmentation, compromises can be made in the adhesion of the dressing to the skin in favor of wearing comfort. Other dressing materials such as upholstery foam or cohesive bandages can then also be used as underlay tape. Polyurethane is typically used to make upholstery foam bandages. Cohesive bandages are usually elastic and self-adhesive thanks to a fine latex coating. However, this adhesion is much less than with adhesive plaster.
investment
In principle, tape dressings are only applied to non-irritated skin. Small wounds can, however, be covered with a suitable wound dressing . In order to achieve sufficient adhesion of the material to the skin, it must first be cleaned sufficiently. Significant pre-tensioning of the adhesive strips or an undersealing tape when applying them (contact pressure) does not improve the adhesion to the skin, but increases the resting pressure of the bandage. In principle, the strips of inelastic plaster are not wrapped continuously like an elastic bandage, but are applied individually in a full wrap.

Liquids such as sweat, grease and oil in particular, but also solid substances such as powder and dirt (e.g. sand or earth) impair adequate adhesion. Excessive hair should also be shaved off beforehand, because on the one hand it reduces the adhesion and on the other hand can lead to unnecessary pain when removing the bandage (without a suitable solvent).
With knowledge of the present diagnosis and the functional anatomical conditions, but also possible alternative treatment options, a tape dressing is theoretically planned in the first step. This includes, on the one hand, the consideration of the course with which the adhesive strip can best augment an injured tape, and on the other hand, an estimate as exact as possible of the strength of the tape bandage in order to adequately fulfill its function. Relatively tight and large-area tape bandages can be applied with greater strength than smaller ones because they distribute the (tensile) forces that occur over larger areas of the skin, but usually also restrict the patient more. Special features of a sport such as the set of rules or, for example, the need not to stick anything on the ball of the big toe in barefoot sports (the fabric strips reduce the grip on the ground), must also be taken into account in these considerations.
construction
After preparation, at least in the case of planned long-term use on sensitive people, an "undersealing tape" should be applied as the first layer to the area of skin intended for the tape bandage. The bandage itself consists of so-called anchor strips , which on the one hand improve the strength of the later bandage and make it easier to put on, of tape reins that simulate the course of the band and can be held in place by fixing strips and also tightened, and of the concluding cladding strips that make up the bandage close and give it additional strength.

storage
Storage is essential for the later stability of a tape bandage. To augment a ligament, a joint is generally positioned in such a way that the corresponding ligament is tensioned as little as possible. The outer band on the upper ankle joint is to say for example in raising the Fußaußenkante and forefoot ( pronation and dorsiflexion treated), the sidebands of the finger joints in slight flexion ( flexion ) and the inner band at the knee joint in flexion easier.
In addition, the patient must be positioned in such a way and, of course, be advised that he does not make any major movements during application, because on the one hand this could thwart an optimal functional result, but on the other hand also to be able to apply the plaster strips without wrinkles.
Follow-up examination
A follow-up examination is necessary once the tape has been applied. In addition to checking the functionality after brief exposure, this also includes an examination and questioning of the patient regarding undesirable symptoms such as pain, numbness or excessive venous congestion.
If the formation of the association is not only planned for the short term (e.g. sporting competition), but for the longer term, the patient should also be informed about possible symptoms that could occur at a later point in time and possible indications of impending complications (see section Complications ).

Decrease
A tape bandage is usually removed by splitting it over its entire length at a suitable point and then pulling it off in the direction of the hair growth.
When splitting the bandage, injuries to the skin should be avoided. Bandage scissors or knives specially made for this purpose by industry , so-called tape cutters , are mostly used. These basically consist of a knife blade with a very blunt back in a fixed holder. However, the cutting edge does not start at the tip of the knife, so that the tape cutter can be pushed forward under the bandage while resting on the skin and splits it from the inside out.
The removal of the bandage can be made easier, especially in the case of pronounced hair growth or sensitive people, by applying suitable solvents (for example, mineral spirits or sprays specially offered by the industry for this purpose). With some products, the plaster strips detach from the adhesive with a slight pull. This then continues to adhere to the skin. Skin irritation from the ingredients of the chemical auxiliaries cannot be ruled out either. However, the pain when removing a large area of tape stuck to the skin is considerably reduced.
Areas of application
Tape bandages are used not only for treatment, but also for reasons of prevention. Depending on the indication , one of the three active principles (compression, splinting as well as augmentation and proprioception improvement) is usually at the fore . As functional bandages, they reduce the mobility of the treated joints, but without completely eliminating them. In addition, they can increase the well-being of athletes in sports. Tape bandages enable experienced physicians to treat many cases on site (e.g. sports facility) in a suitable manner using easily and quickly available self-adhesive plaster strips. In the case of longer-term applications and the foreseeable necessary complete renewal of the dressing, other aids, such as orthoses, can be more cost-effective.
Prevention
In order to avoid sports injuries in particular, tape bandages are customary in many different sports, such as handball , basketball , sport climbing , taekwondo and windsurfing , and not only in competitive sports . In order to be able to prevent overstretching of the ligaments, they are usually put on quite tightly and must therefore be removed again promptly after a competition.
Tape bandages are used for prevention in uninjured athletes, but are also particularly suitable after injuries have healed in order to reduce the risk of renewed, similar injuries. The investigations carried out for the upper ankle joint over the past five decades, for example, have produced corresponding results. However, a large-scale, prospective , randomized study is still lacking. If the rules of the respective sport permit, orthoses available in stores can also be used as an alternative. The reasons for this are that these can often be put on more quickly and without much specialist knowledge, but at the same time have a preventive effect that is quite comparable to the tape dressing.
Tape dressings intended solely for prevention are not considered therapy in the actual sense and can also be put on by a suitably trained physiotherapist or the (competent) athlete himself.
therapy
Tape bandages are used both after acute injuries and for their follow-up treatment. These include lesions of the capsule-ligament apparatus of joints , unless other procedures such as surgical measures or immobilization in a plaster cast are absolutely necessary, but also chronic joint instabilities , some simple bone fractures, muscle injuries and also damage caused by overuse such as the thrower's wrist . The therapeutic efficiency of tape dressings is generally recognized for injuries to the outer ligament of the ankle. In the case of fractures of the head of the fifth metacarpal bone , the effectiveness of tape dressings is equivalent to that of other therapeutic methods ( e.g. reduction and spiked wire osteosynthesis ). With heel spurs and impingement syndrome of the shoulder as well as dislocation of a long middle finger joint (so there basically always associated injuries of the capsule ligament apparatus), this shall also be established therapeutic measures are. When Running tape dressings are suitable stress-related knee pain ( knee runner's ) within the range of Reduce femoral patellar (retropatellar) plain bearing .
performance increase
Taping the ankle can lead to significant increases in performance in the Fosbury flop through so-called proprioception improvement and the possibility of using muscle power against resistance (similar to a weight lifting belt) . Taping in American football and boxing is based on similar principles , where the fists are taped under the gloves.
Possible applications
Tape bandages are usually applied to the arms or legs, but can also be used on the trunk of the body . They are not only described for the hand and fingers, feet and toes, the large joints of the extremities (elbows, shoulders and knees) as well as the spine and thorax, but also, for example, for the muscles of the lower and upper legs.
The bandages are generally planned and applied individually for each patient. Their specific implementation depends on the localization and is based on the purpose (prevention or therapy), the planned duration for which the dressing is to be left on, and the active principle or principles intended for the application (compression, splinting, as well as augmentation and proprioception improvement). (A few examples are shown below.)
Lateral ligament of a long finger middle joint

Bones and ligaments of a long finger

Representation of the side ligaments


The middle joints of the long fingers are hinge joints , their mobility is reduced to flexion and extension under physiological conditions. They cannot actively turn or move sideways. Your capsule-band device is designed accordingly.

If a lateral force acts on one finger joint, tensile forces occur in the opposite side ligament. An injury occurs when these tensile forces exceed the belt stability. The potential extent of the ligament injury ranges from a slight strain to a complete tear . In addition to swelling and bruising in the area of the injury, the consequences can also be instability of the joint and pain if tensile forces occur again in the injured collateral ligament. Such lesions lead to more or less pronounced functional restrictions of the hand, since tensile forces in the side ligaments also occur during normal gripping and holding movements (for example, catching a ball).
As therapy recommendations for a complete rupture of the collateral ligament of a long finger medial joint (exception is the radial, i.e. thumb-side ligament on the index finger), in addition to surgical measures and immobilization, tape bandages can also be found in the literature. The latter are also recommended for all incomplete ruptures . Alternatively, orthoses and, in the case of complete ruptures, surgical measures are also used.

The shining tape bandage essentially consists of two reins that connect the base and middle phalanx of the injured and the uninjured neighboring finger (buddy taping) . The distances between the plaster strips and the middle joint should be roughly the same in order to avoid unnecessary skin irritation caused by tensile forces. Padding between the fingers is mandatory. Typically, the finger on the injured side is included in the bandage. This tape bandage only slightly restricts the mobility of both fingers. If it is put on when the rupture is incomplete, the patient can then resume training with handball and basketball. In these cases, the bandage is left in place for about three weeks and then applied for about half a year during sporting activities.
In the case of simple distortions of the collateral ligament, an augmenting tape bandage on the affected finger is sufficient . Ensure that the plaster strips adhere well to the skin. The bandage extends from the base joint to the fingernail, its stabilizing effect is achieved by longitudinal and semi-circular reins.
- Augmenting tape on the finger

Semi-circular reins

Longitudinal reins

Complete tape dressing with anchor and formwork strips (stretching is possible)



Thrower wrist
The thrower's or gymnast's wrist occurs as a result of excessive strain on the wrist caused by sports. Microtraumas and mechanical entrapment in the event of forced, maximum dorsiflexion (hyperextension) are considered to be the cause and should therefore be avoided during treatment. The task of a suitable tape dressing is to prevent this excessive overstretching. It is to applied in a slight flexion of the wrist so that the reins tape (similar to the finger middle joint semizirkulär) come when stretched under the train and so the capsular ligaments of the joint augment to prevent hyperextension.
- Position and function of the outer ligaments
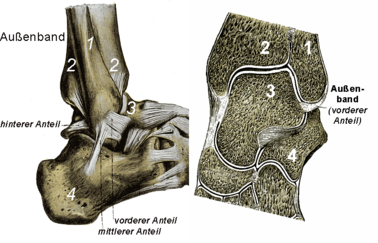
Left: side view of the external ligament apparatus with its three parts.
Right: Cross-section at the level of the front part of the outer band.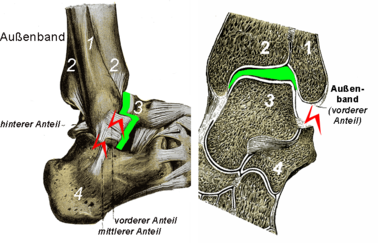
Left external ligament instability : The talus can be pulled forward.
Right: The upper ankle can be opened to the side.


External ligament at the ankle
Tape bandages are used on the outer ligament of the upper ankle joint for recent injuries, but also for permanent ligament weaknesses.
Fresh injuries are divided into three groups (degrees). These include mere sprains without any evidence of weakness in the ligamentous apparatus, partial tears in one or more parts of the outer ligament, and complete ruptures. The cause of such injuries is usually a so-called supination trauma , i.e. a twisting of the ankle with the foot pointing outwards.
The most common cause of a permanently loose ligament system is insufficiently healed ligament injuries. Chronic instability, especially during sport, leads to frequent twisting of the foot outwards and thus to osteoarthritis due to repeated microtraumas of the articular cartilage .
Augmenting tape dressings can be used to treat recent injuries of all degrees as well as chronic ligament instabilities. They are to be applied tightly and with good adhesion to the skin, especially since it has been known for many decades that they quickly (10 minutes) lose 40 to 50 percent of their stability during exercise. The plaster strips have to be stuck on in such a way that they support the function of the outer ligament apparatus by preventing the lateral opening and advancement of the ankle bone as much as possible.

There are numerous indication-related suggestions for the specific procedure. Basically, after a corresponding examination of the joint, the optimal course of the plaster strips is chosen to counteract the instability and thus to augment the outer ligament apparatus. In order to achieve maximum stability, the bandage begins just below the knee joint and ends at the metatarsophalangeal joints. Shorter bandages are less stable, but are used as a preventative measure in previously healthy athletes because of their comfort. When putting on, the foot is placed in pronation and dorsiflexion. The main tape reins run slightly diagonally from the lower leg to the foot, to which they are attached in a semi-circular manner. This creates a gap between the ankle region and the plaster strip. These are then tightened by means of fixing strips that run approximately at right angles to them and are glued to the skin over the area of the outer ankle. The reins must be pre-tensioned so that the bandage achieves sufficient stability even during prolonged sporting activities.
- Lateral and anterior instability at the knee joint (diagram)
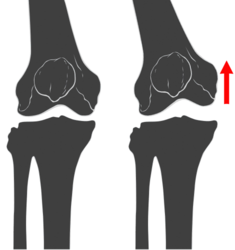
Medial instability (assessment depends on the knee joint position)

Anterior drawer (often accompanying weakness of the anterior cruciate ligament)


Inner ligament of the knee joint
Under physiological conditions, the knee joint is stabilized medially (on the inside) not only by the inner ligament, but also by other structures of its capsule-ligament apparatus. However, the contribution of the individual structures to the stabilization depends on the angular position of the joint. In the extended position, for example, the anterior cruciate ligament is much more involved than in 30-degree flexion. If the knee joint is medially unstable during the clinical examination in the extended position, i.e. if the joint gap can be opened, this is usually not only due to an inadequacy of the holding function of the inner ligament, but also of the anterior cruciate ligament, for example. The latter also stabilizes the shin on the thigh bone, thus preventing the head of the shin from sliding forward. If the anterior cruciate ligament is weak, the tibia can be pulled a little forward during the examination (anterior drawer) . One then speaks of an anterior-medial instability.

The cause for this is usually a valgus trauma, i.e. a force acting on the knee joint from the lateral side (from the outside). This accident mechanism can, depending on the joint position in the accident and the resulting torsional forces, lead to an unhappy triad even in very pronounced cases . Therapy and follow-up treatment of isolated injuries of the inner ligament are carried out functionally conservatively using orthotics and tape bandages, regardless of whether it is a strain (grade I) or a complete rupture (grade III).
The augmenting tape dressing on the knee joint is placed in a slightly flexed position. In this position, even in healthy athletes, the holding function of the inner ligament is least supported by other structures (prevention). In addition, an accompanying anterior instability ( anterior cruciate ligament ) can also be included in this position . The reins of the tape bandage run from the inside of the thigh to the lower leg, to which they are attached in a semi-circular manner. An additional tightening (as on the outer ankle) is hardly possible for anatomical reasons. If there is a clinically conspicuous anterior drawer , additional reins are applied laterally analogously.

Metatarsal fracture
Fractures of one of the five metatarsal bones occur during exercise with and without trauma .
If indicated, a very simply structured , seeming tape bandage is applied, which consists only of circular (around 360 °) strips of plaster applied to the unloaded forefoot. This allows the forefoot when can occur less deform significantly. This is because the circle is the shortest boundary of an area. Since the forefoot is forced into the shape of a cylinder by the tightly applied tape bandage , it can hardly change its shape, since any other shape would require a larger circumference. Under normal conditions, a tape bandage splinters the injured bones. Similar tape bandages are also used preventively in sports.

Hammer toe
As Hammer , strictly speaking, refers to a toe (usually the 2nd or 3rd), the distal interphalangeal joint (DIG) and in some cases, the middle joint (PIG) is a more or less pronounced contracture has. Hammer toes lead to clav formation and impair walking due to pain in the shoe. The distinction between hammer and claw toes is not clear in all cases. The causal factors are diverse, inadequate footwear is typical for athletes. In severe cases with fixed joint deformities, surgical measures are indicated; in mild cases, in which the deformity can still be passively compensated, a tape bandage (possibly together with a night correction splint) may be sufficient.
The function of the tape bandage is to support the (actively lost) extension of the toe joint. After passive extension of the joint, this joint position is fixed with adhesive tape. Several stripes run from the toe berry over the back of the toe and the forefoot to the Achilles tendon . The toe is fixed in the extended position by the adhesive tape adhering to the skin (augmentation).
Lower leg muscles
Tape bandages are used for fresh, but also for past injuries to the muscles of the lower leg, such as muscle strains and torn muscle fibers . In the case of fresh injuries, the compressing tape bandage is indicated as an initial measure. To do this, the lower leg and, if necessary, the foot are first wrapped with an undersurface tape, which is easily detached from the skin when the tape bandage is changed and thus enables multiple, short-term changes without significant skin irritation. The inelastic adhesive plaster strips are then applied without any significant pressure so that a compression bandage is created without resting pressure, but with maximum working pressure. The adhesion to the skin only needs to be so great that the bandage does not slip without the patient doing something.
To some extent one is augmentation of the injured muscle by means of taping possible. For this purpose, the plaster strips are glued in a semicircular, diagonal manner directly to the skin or alternatively on a well-adhering undersurface tape.
Complications

Typical signs of possible complications with tape bandages are itching , pain , swelling, numbness or abnormal sensations such as tingling and disorders of the blood circulation .
Skin irritation
Adhesives based on zinc oxide , rubber or resin are particularly likely to cause skin irritation. Those based on polyacrylate or fumaric acid ester are considered to be better tolerated . Cleaning agents can also cause skin irritation , especially if there are still residues when a tape dressing is put on (for example, wound gasoline or disinfectant that has not completely evaporated ).
However, irritation to the skin can also be caused by mechanical factors. They occur when the tensile forces that the tape dressing exerts on the skin are greater than they can compensate for due to their mobility. This results in tiny cracks in the horny layer of the skin . Another mechanical cause is too frequent changing of the tape dressing. Each time the bandage fixed on the skin by means of adhesive is removed, the superficial parts of the horny layer are also removed. This is thinned out, loses its mechanical strength and can therefore withstand the tensile forces less.

Loss of effectiveness
The main reason for the loss of effectiveness of a correctly applied tape dressing is a decrease in adhesion to the skin. The causes of this are normal peeling of the horny layer and sweat. If the sweat glands produce more fluid than can be absorbed by the bandage and transported to the outside , small fluid cushions are created around their ducts ( pores ), which over time raise the bandage again and again and thus reduce its adhesion to the skin.
Compartment syndrome
If a tape dressing leads to a significant congestion of the venous return flow, a compartment syndrome can occur if it is left on for too long. Venous congestion increases the pressure of the blood in the veins and thus in the tissue.
literature
- A. Schur: Taping: Use in sports. Meyer & Meyer Verlag, 2009, ISBN 978-3-89899-567-2 .
- H. Mommsen: Right taping. Optimally apply functional bandages to the musculoskeletal system: the balance between stability and mobility. Spitta Verlag, 2007, ISBN 978-3-934211-46-9 .
- K. Price: Tape dressings in sports medicine: Notes on the technique of applying tape dressings. Hartmann Verlag, 1993, ISBN 3-929870-03-7 .
- C. Lukas et al: Ankle injuries in basketball: background, therapy and prophylaxis. Books on Demand Verlag, 2010, ISBN 978-3-8391-7201-8 .
Individual evidence
- ↑ A. Braun: Foot: Diseases and Injuries. (= Volume 39 of the conference of the professional association of doctors for orthopedics e. V, professional association of doctors for orthopedics). Verlag Birkhäuser, 1999, ISBN 3-7985-1190-X , pp. 126-128, online
- ↑ a b R. W. Poolman et al .: Conservative treatment for closed fifth (small finger) metacarpal neck fractures. In: Cochrane Database of Systematic Reviews. 2005, Issue 3. Art. No .: CD003210. doi: 10.1002 / 14651858.CD003210.pub3 , online
- ↑ a b c d e f J. Durst: Traumatological practice: in one volume: standards in diagnostics and therapy for all specialist areas. Schattauer Verlag, 1997, ISBN 3-7945-1587-0 , pp. 24-26, online
- ↑ a b H. Lohrer et al.: Injuries to the lateral capsular ligament apparatus of the ankle - an overview. In: German magazine for sports medicine. 2000/6, ISSN 0344-5925 , pp. 196–203, pdf ( page no longer available , search in web archives ) Info: The link was automatically marked as defective. Please check the link according to the instructions and then remove this notice.
- ↑ a b S. Robbins et al: Ankle taping improves proprioception before and after exercise in young men. In: Br J Sports Med. 1995; 29, pp. 242-247 doi: 10.1136 / bjsm.29.4.242 , online
- ^ DA McLean: Use of adhesive strapping in sport. In: Br J Sports Med. 1989 September; 23 (3), pp. 147–149, PMC 1478673 (free full text)
- ↑ a b T. Noppeney among others: Varicosis: Diagnostic-Therapy-Assessment. Springer, 2010, ISBN 978-3-642-05365-8 , pp. 230ff., Online
- ^ I. Blank: Wound care and dressing change. W. Kohlhammer Verlag, 2007, ISBN 978-3-17-019162-4 , p. 168, online
- ↑ a b H. J. Montag, PD Asmussen: Taping seminar. Spitta Verlag, 1995, ISBN 3-929587-44-0 , pp. 42-43.
- ↑ a b c d J. C. DeLee, D. Drez: Orthopedic Sports Medicine. Saunders, Philadelphia 1994, ISBN 0-7216-2836-2 , pp. 961ff.
- ↑ David Maraniss: Rome 1960: The Olympics That Changed the World. Simon & Schuster, New York 2008, ISBN 978-1-4165-3407-5 , pp. 287f.
- ↑ K. O'Sullivan et al .: The effect of low-dye taping on rearfoot motion and plantar pressure during the stance phase of gait. In: BMC Musculoskelet Disord. 2008; 9, p. 111, PMC 2529302 (free full text)
- ↑ A. Derasari et al .: McConnell Taping Shifts the Patella Inferiorly in Patients With Patellofemoral Pain: A Dynamic Magnetic Resonance Imaging Study. In: Phys Ther. 2010 March; 90 (3), pp. 411–419, PMC 2836141 (free full text)
- ^ J. McConnell et al .: The Effect of Tape on Glenohumeral Rotation Range of Motion in Elite Junior Tennis Players. In: Clinical Journal of Sport Medicine. March 2009, Volume 19, Issue 2, pp. 90-94, online
- ↑ a b T. Carver: Ankle Positioning in Ankle taping of Swimmers. In: J Athl Train. 1992; 27 (3), pp. 270, 272, PMC 1317259 (free full text)
- ↑ Competition rules of the German Taekwondo Union (as of September 16, 2002), Paragraph 5.9.2.1, pdf ( memento of the original from September 19, 2011 in the Internet Archive ) Info: The archive link was inserted automatically and has not yet been checked. Please check the original and archive link according to the instructions and then remove this notice. ; last viewed on September 1, 2010.
- ↑ V. Schöffl et al.: Differential diagnosis of finger pain in sport climbers. In: German magazine for sports medicine. Süddeutscher Verlag onpact, 2003/2, ISSN 0344-5925 , pp. 38-42, pdf
- ↑ K. Knobloch among others: Basketball injuries in school sports. In: German magazine for sports medicine. Süddeutscher Verlag onpact, 2005/4, ISSN 0344-5925 , pp. 96-99, pdf ( page no longer available , search in web archives ) Info: The link was automatically marked as defective. Please check the link according to the instructions and then remove this notice.
- ↑ H. Rieckert include: Sports medical aspects of windsurfing. In: Dtsch Arztebl. 2001; 98 (1-2), pp. A-39 / B-35 / C-35, online
- ↑ C. Lauren et al .: Prophylactic Ankle Taping and Bracing: A Numbers-Needed-to-Treat and Cost-Benefit Analysis. In: J Athl Train. 2004 Jan – Mar; 39 (1), pp. 95-100, PMC 385268 (free full text)
- ↑ C. Richard et al .: A Comparison of Moleskin Tape, Linen Tape, and Lace-Up Brace on Joint Restriction and Movement Performance. In: J Athl Train. 1997 Apr-Jun; 32 (2), pp. 136–140, PMC 1319816 (free full text)
- ↑ a b appeal H.-J. among others: textbook of sports medicine. Deutscher Ärzteverlag, 2001, ISBN 3-7691-7073-3 , p. 221, online
- ^ A b S. Maibaum et al.: Therapy lexicon of sports medicine: treatment of injuries to the musculoskeletal system. Springer, 2001, ISBN 3-540-66759-8 , pp. 19, 44ff, 89, 125, 205, online
-
↑ JG Garrick et al: Role of external support in the prevention of ankle sprains. In: Med. Sci. Sports Exerc. 1973, 5, pp. 200-203;
R. Bahr et al .: Biomechanics of ankle ligament reconstruction. In: Am. J. Sports Med. 26 (1997), pp. 424-432;
W. Alt et al .: Proprioceptive effect in ankle stabilization aids. In: Orthopädieschuhtechnik 2 (1999), pp. 30-36;
W. Alt ua: Doesn't tape work !? Proprioceptive and mechanical studies on the effectiveness of stabilizing tape dressings on the ankle. In: Sportorthop. Sports trauma. 14: 75-85 (1998);
W. Alt et al .: Functional properties of adhesive ankle taping: neuromuscular and mechanical effects before and after exercise. In: Foot & Ankle Intern. 20 (1999), pp. 238-245;
quoted from: H. Lohrer et al.: Injuries to the lateral capsular ligament apparatus of the ankle joint - an overview. In: German magazine for sports medicine. Volume 51, No. 6 (2000), pp. 196–203, pdf ( page no longer available , search in web archives ) Info: The link was automatically marked as defective. Please check the link according to the instructions and then remove this notice. - ↑ HR Osborne et al: Treatment of plantar fasciitis by LowDye taping and iontophoresis: short term results of a double blinded, randomized, placebo controlled clinical trial of dexamethasone and acetic acid. In: Br J Sports Med. 2006 June; 40 (6), pp. 545–549, PMC 2465091 (free full text)
- ↑ P. Miller et al .: Does Scapula Taping Facilitate Recovery for Shoulder Impingement Symptoms? A Pilot Randomized Controlled Trial. In: J Manip Ther. 2009; 17 (1), pp. E6 – E13, PMC 2704341 (free full text)
- ^ A. Freiberg: Management of proximal interphalangeal joint injuries. In: Can J Plast Surg. 2007 winter; 15 (4), pp. 199–203, PMC 2696003 (free full text)
- ^ H. Dickhuth et al.: Injuries and complaints in running: prevention and therapy. In: Dtsch Arztebl. 2001; 98 (19), pp. A-1254 / B-1069 / C-997, online
- ↑ Gharavi-Nouri, Homayun: The tape bandage on the ankle as a technical component to improve performance in sport using the example of the Fosbury flop: a training-based study on high jumpers. Diss. Univ. Göttingen 2005. https://opac.sub.uni-goettingen.de/DB=1/SET=4/TTL=1/CMD?ACT=SRCHA&IKT=1016&SRT=YOP&TRM=tape+fosbury&MATCFILTER=N&MATCSET=N&NOSCAN=N&ADI_BIB=
- ^ HJ Montag, PD Asmussen: Taping seminar. Spitta Verlag, 1995, ISBN 3-929587-44-0 , pp. 10-11.
- ↑ V. Schöffl: Hand injuries while climbing. In: German magazine for sports medicine. Süddeutscher Verlag onpact, 2008/4, ISSN 0344-5925 , pp. 85–90, pdf ( page no longer available , search in web archives ) Info: The link was automatically marked as defective. Please check the link according to the instructions and then remove this notice.
- ↑ U. Wegner: Sports injuries: symptoms, causes, therapy. Verlag Schlütersche, 2002, ISBN 3-87706-632-1 , p. 82, online
- ↑ a b J. C. DeLee, D. Drez: Orthopedic Sports Medicine. Saunders, Philadelphia 1994, ISBN 0-7216-2836-2 , pp. 1705ff.
- ↑ GL Rarick et al .: The Measurable Support of the Ankle Joint by Conventional Methods of Taping. In: J Bone Joint Surg Am . 1962; 44, pp. 1183–1190, pdf ( page no longer available , search in web archives ) Info: The link was automatically marked as defective. Please check the link according to the instructions and then remove this notice.
- ^ HJ Montag, PD Asmussen: Taping seminar. Spitta Verlag, 1995, ISBN 3-929587-44-0 , pp. 68-88.
- ↑ JC DeLee, D. Drez: Orthopedic Sports Medicine. Saunders, Philadelphia, 1994, ISBN 0-7216-2836-2 , pp. 1261ff.
- ↑ H.-J. Appeal among other things: textbook of sports medicine. Deutscher Ärzteverlag, 2001, ISBN 3-7691-7073-3 , p. 302.
- ↑ a b K. J. Munzenberg: Orthopedics in practice. VCH-Verlag, 1988, ISBN 3-527-15320-9 , pp. 172-3.
- ^ A b B. H. Reuter: Taping the Hammer Toe. In: J Athl Train. 1995 June; 30 (2), pp. 178-179., PMC 1317854 (free full text)
- ^ HJ Montag, PD Asmussen: Taping seminar. Spitta Verlag, 1995, ISBN 3-929587-44-0 , pp. 119-123.